
REGDOC-2.7.2, Dosimetry, Volume I: Ascertaining Occupational Dose
View or download as a PDF [96 pages, 2.32 MB]
Preface
This regulatory document is part of the CNSC’s radiation protection series of regulatory documents. The full list of regulatory document series is included at the end of this document and can also be found on the CNSC’s website.
Regulatory document REGDOC-2.7.2, Volume I, sets out guidance for ascertaining occupational dose. It also provides guidance for making changes to dose-related information filed with Health Canada’s National Dose Registry.
For information on the implementation of regulatory documents and on the graded approach, see REGDOC-3.5.3, Regulatory Fundamentals.
The words “shall” and “must” are used to express requirements to be satisfied by the licensee or licence applicant. “Should” is used to express guidance or that which is advised. “May” is used to express an option or that which is advised or permissible within the limits of this regulatory document. “Can” is used to express possibility or capability.
Nothing contained in this document is to be construed as relieving any licensee from any other pertinent requirements. It is the licensee’s responsibility to identify and comply with all applicable regulations and licence conditions.
Table of Contents
- 1. Introduction
- 2. General Information
- Part A – External Exposure
- 3. Operational Dose Quantities
- 4. Direct Monitoring
- 5. Ascertaining External Dose Through Estimation
- Part B – Internal Exposure
- 6. Quantities
- 7. Intake Monitoring Methods
- 8. Interpreting Monitoring Results
- 9. Ascertaining the Committed Effective Dose
- 10. Calibration
- 11. Limiting Intakes of Nuclear Substances by Workers Who Are Breastfeeding
- 12. Ascertaining the Dose Resulting From an Intake of Nuclear Substances via a Wound
- Part C – Making Changes to Dose-Related Information Filed With the National Dose Registry
- 13. General Process
- 14. Individual Dose Information Change Request Procedure
- 15. Group Dose Information Change Request Procedure
- 16. Contact Information
- Appendix A: Guidance on Choosing Dosimetry for the Lens of the Eye
- Appendix B: Assessing the Activity Handled for Selecting Participants in a Routine Intake Monitoring Program
- Appendix C: Bioassay Protocols for Responding to Abnormal Intakes of Radionuclides
- Appendix D: Radionuclide-Specific Recommendations Related to Bioassay Measurements and Internal Dosimetry – Tritium
- Appendix E: Radionuclide-Specific Recommendations Related to Bioassay Measurements and Internal Dosimetry – Radioiodines
- Appendix F: Radionuclide-Specific Recommendations Related to Bioassay Measurements and Internal Dosimetry – Uranium
- Appendix G: Radionuclide-Specific Recommendations Related to Air Monitoring and Internal Dosimetry – Radon progeny
- Glossary
- References
- Additional Information
1. Introduction
Regulatory document REGDOC-2.7.2, Dosimetry, Volume I: Ascertaining Occupational Dose, updates and supersedes the following previously published regulatory documents on dosimetry‑related topics:
- G-91, Ascertaining and Recording Radiation Doses to Individuals (2003)
- G-147, Radiobioassay Protocols for Responding to Abnormal Intakes of Radionuclides (2003)
- RD-58, Thyroid Screening for Radioiodine (2008)
- GD-150, Designing and Implementing a Bioassay Program (2010)
- S-260, Making Changes to Dose-Related Information Filed with the National Dose Registry (2004)
New guidance is provided on the following topics:
- ascertainment and recording of the equivalent dose to the lens of the eye
- use of licensed dosimetry services for annual doses to the skin, or to the hands and feet, greater than 50 mSv
The document is divided into 3 parts:
- Part A provides information on ascertaining occupational dose from external sources of radiation.
- Part B provides information on ascertaining occupational dose from internal sources of radiation.
- Part C describes the process for making changes to dose-related information filed with the National Dose Registry (NDR).
1.1 Purpose
REGDOC-2.7.2, Volume I, provides guidance for ascertaining occupational dose. It also provides guidance for making changes to dose-related information filed with the NDR.
1.2 Scope
This document provides guidance for dosimetry to ensure the protection of workers. The scope of this document does not include:
- guidance for radiation protection, which is provided in REGDOC 2.7.1, Radiation Protection [1]
- requirements and guidance for dosimetry services, which are provided in REGDOC-2.7.2, Dosimetry, Volume II: Technical and Management System Requirements for Dosimetry Services [2]
- requirements and guidance relating to environmental protection, which are provided in REGDOC‑2.9.1, Environmental Principles, Assessments and Protection Measures [3]
1.3 Relevant legislation
The following provisions of the Nuclear Safety and Control Act (NSCA) are relevant to this document:
- Section 2 defines the term nuclear energy worker (NEW).
- Section 27 states that licensees must keep dose records and retain them for a prescribed amount of time.
The following provisions of the Radiation Protection Regulations (RPR) are relevant to this document:
- Subsection 5(1) requires every licensee to ascertain and record the magnitude of exposure to radon progeny of each person referred to in section 27 of the NSCA, as well as the effective dose and equivalent dose received by and committed to that person.
- Section 13 sets effective dose limits.
- Section 14 sets equivalent dose limits.
- Section 15 sets dose limits for persons participating in the control of an emergency.
- Subsection 24(2) states that licensees must maintain dose records for a period of 5 years after the day the information is collected.
2. General Information
2.1 Effective dose limits
The regulatory limits on effective dose apply to all sources of radiation exposure combined, that is, to sources external to the body and to sources within the body.
Section 13 of the RPR sets out the effective dose limits to various persons. These persons are NEWs, pregnant NEWs, and persons who are not NEWs. Section 15 of the RPR sets out effective dose limits for persons participating in the control of emergencies.
For each of these persons, the effective dose limits apply to the sum of:
- the effective dose received from sources of ionizing radiation outside the body
- the committed effective dose (CED) from radon and radon progeny, when taken into the body
- the CED from radionuclides (other than radon-222 and its progeny) taken into the body
The total effective dose, as determined by the above summation method, is compared with the applicable effective dose limits, stipulated in sections 13 and 15 of the RPR, to determine compliance with those limits.
2.2 Equivalent dose limits
Section 14 of the RPR sets out the equivalent dose limits to NEWs and any other person for the lens of the eye, skin, and hands and feet. Section 15 of the RPR sets out equivalent dose limits for persons participating in the control of emergencies. For each of these persons, the equivalent dose limits apply to the product, in sieverts, obtained by multiplying the absorbed dose by the weighting factor of a given type of radiation.
The equivalent dose, as determined by the method above, is compared with the applicable equivalent dose limits, stipulated in sections 14 and 15 of the RPR, to determine compliance with those limits.
2.3 Dosimetry methods
This document refers to 3 general approaches to dosimetry: direct monitoring, indirect monitoring and dose modelling.
Direct monitoring refers to personal dosimetry or individual monitoring. It includes the use of personal whole-body or extremity dosimeters, personal air samplers, as well as in vivo and in vitro bioassay measurements. Direct monitoring is the most accurate and preferred method to ascertain doses to workers.
Indirect monitoring refers to workplace monitoring. It includes area gamma or neutron dose rate measurements and area air monitoring. Workers’ doses may be estimated by applying indirect monitoring results to their occupancy times.
Dose modelling refers to estimating doses on the basis of a characterized source term, taking into account relevant parameters such as exposure time and geometry, shielding, type of radiation, or nuclear substance. It includes the application of published dose coefficients, is typically carried out by using software, and is generally prospective in nature. The sources of dose coefficients typically include those published by the International Commission on Radiological Protection (ICRP). It should be noted that the ICRP internal dose coefficients are being updated to incorporate the tissue weighting factors introduced in ICRP Publication 103, The 2007 Recommendations of the International Commission on Radiological Protection [4]. However, the use of current ICRP dose coefficients remains acceptable at this time for the purposes of dose modelling.
2.4 Dosimetry services
Section 8 of the RPR requires licensees to use a dosimetry service that is licensed by the CNSC to measure and monitor the doses of radiation received by and committed to NEWs who have a reasonable probability of receiving:
- an effective dose greater than 5 mSv in a 1-year dosimetry period, or
- an equivalent dose to the skin, or to the hands and feet, that is greater than 50 mSv in a 1‑year dosimetry period
This requirement ensures that doses are monitored with sufficient accuracy and precision. Requirements relating to licensed dosimetry services can be found in REGDOC-2.7.2, Volume II [2].
Guidance on determining when licensed dosimetry would be required can be found in REGDOC‑2.7.1 [1].
2.5 Dose records
All data used to ascertain doses, reports generated as part of investigations, and documents associated with dose change requests (DCRs), including the investigation report, the DCR form and the CNSC approval letter, must be kept for the period of time prescribed in subsection 24(2) of the RPR. Such data should enable reasonable re-creation and checking of results from referenced input data. A clear method to identify workers and maintain dose records should be established. The identification, storage, protection, retrieval and disposition of records should be controlled.
2.6 National Dose Registry
According to the RPR, if dose measurements are recorded by a licensed dosimetry service, dose records for NEWs are required to be submitted to the NDR along with specific personal information identified in the RPR.
The NDR is a database owned and operated by Health Canada that tracks the lifetime dose history of registered individuals. The CNSC has a memorandum of understanding with Health Canada that sets out Health Canada’s responsibility to operate the registry, maintain the information required under the RPR and make that information available to the CNSC. Footnote 1
Upon request, Health Canada shares information from the NDR with the CNSC. This includes information on trends relating to dose data for facilities or groups of facilities; detailed dose information for individuals and licensees; and necessary information for the conduct of health studies, including epidemiological studies. Health Canada also informs the CNSC of any records indicating that a dose limit for a NEW has been exceeded. Prompt identification of such records allows the CNSC to act immediately to ensure that licensees have taken appropriate action as required by the RPR.
A licensee may request a change to a dose record or changes to a group of dose records in the NDR. Part C describes the process for making changes to dose-related information filed with the NDR.
2.7 Characterization of radiological conditions
A workplace hazard assessment should be carried out and documented. Consequently, the radiological conditions (e.g., facility layout, types of radionuclides and activities being undertaken) at a licensed facility or at a location where a licensed activity is being carried out should be characterized, documented, monitored, and updated in the event of changes that may impact doses to workers. Characterization of radiological conditions should provide a comprehensive description of radiation sources and the nature of radiation present in all work locations that may result in occupational exposure. The radiological conditions should be verified periodically and the documentation should be kept up to date.
For sources of external exposure, radiological characterization should include:
- the radionuclides expected to be present at the workplace, as well as their half-life, progeny and relative abundances
- the radiation types and energies emitted by those radionuclides
- a description of radiation sources (e.g., physical form, geometry and applicable shielding information)
If applicable, licensees should document the neutron energy spectrum at their workplace. This information should be used to select suitable methods for ascertaining occupational dose from neutron exposures. Generally, characterization of radiological conditions in a workplace provides important information to select appropriate types of dosimetry.
For sources of internal exposure, the radiological characterization should provide a comprehensive description of the nature, extent and variability of surface contamination, airborne radioactivity and other potential sources of intakes, as appropriate, at all work locations. The radiological characterization should document default values and, where applicable, the following information, for all locations in a facility:
- the radionuclides expected to be present at the workplace, as well as their half-life, progeny and relative abundances
- the radiation types and energies emitted by those radionuclides
- their chemical forms and related respiratory tract clearance types
- the particle size (expressed as the activity median aerodynamic diameter, or AMAD), if applicable
Part A – External Exposure
External dosimetry is the measurement of dose when radiation sources are outside the body. External dosimetry is concerned with radiation that can penetrate the dead layer of skin: photon, beta and neutron radiation. Since photons and betas result in charged particle interactions and neutrons interact through nuclear forces, their dosimetry and the methods for detecting them are substantially different.
External exposure to radiation can be measured by direct monitoring. However, if the time and resources required for direct measurement outweigh the usefulness of that method, the exposure can be estimated.
3. Operational Dose Quantities
Operational dose quantities are defined in the International Commission on Radiation Units and Measurements (ICRU) Report 51, Quantities and Units in Radiation Protection Dosimetry [5], as a set of measurable quantities of external exposures that can be used to demonstrate compliance with regulatory dose limits. The following information is based on that report.
3.1 Ambient dose equivalent, H*(d)
The ambient dose equivalent is used when area monitoring is used to ascertain external dose. For strongly penetrating radiation, a depth of 10 mm is used. For weakly penetrating radiation, depths of 0.07 mm for the skin and 3 mm for the lens of the eye are used. H*(d) represents the ambient dose equivalent, where (d) is the depth measured in millimetres.
3.2 Directional dose equivalent, H’(d, Ω)
The directional dose equivalent is used when area monitoring is used to ascertain external dose. This operational quantity takes into consideration the specified direction of the radiation field, Ω. For strongly penetrating radiation, a depth of 10 mm is used. For weakly penetrating radiation, depths of 0.07 mm for the skin and 3 mm for the lens of the eye are used. H’(d, Ω) represents the directional dose equivalent, where d is the depth measured in millimetres.
3.3 Personal dose equivalent Hp(d)
The personal dose equivalent is the operational quantity employed when direct (or individual) monitoring is used to ascertain external dose. For strongly penetrating radiation, a depth of 10 mm is used. For weakly penetrating radiation, depths of 0.07 mm for the skin and 3 mm for the lens of the eye are used. Hp(d) represents the personal dose equivalent, where (d) is the depth measured in millimetres.
| Operational quantity | Description |
|---|---|
| H*(10) | Ambient dose equivalent at 10 mm depth |
| H*(0.07) | Ambient dose equivalent at 0.07 mm depth |
| H*(3) | Ambient dose equivalent at 3 mm depth |
| H’(10, Ω) | Directional dose equivalent at 10 mm depth |
| H’(0.07, Ω) | Directional dose equivalent at 0.07 mm depth |
| H’(3, Ω) | Directional dose equivalent at 3 mm depth |
| Hp(10) | Personal dose equivalent at 10 mm depth |
| Hp(0.07) | Personal dose equivalent at 0.07 mm depth |
| Hp(3) | Personal dose equivalent at 3 mm depth |
4. Direct Monitoring
In order to ascertain external doses to workers, direct monitoring may be carried out using a personal dosimeter. Worker doses may be ascertained using dosimetry provided by a licensed dosimetry service. Alternatively, when licensed dosimetry is not required, doses may be ascertained by direct monitoring techniques specified in the licensee’s radiation protection program.
Dosimeters are classified into 2 general categories:
- passive dosimeters, which produce a radiation-induced signal that is stored in the device (the dosimeter is then processed and the output is analyzed)
- active dosimeters, which produce a radiation-induced signal and display a direct reading of the detected dose or dose rate
A typical passive dosimeter used to measure photon and beta radiation consists of a detector inserted into a holder. Dosimeters vary in their configuration. However, the detector contains the sensitive element(s) and the holder contains the filter(s). In a dosimeter that measures photon and beta radiation, it is mainly the filter/holder that permits the instrument to differentiate between the personal dose equivalent to the skin or eye (Hp(0.07) and Hp(3) respectively) and the personal dose equivalent to the whole body (Hp(10)). One part of the holder may have an open window (no filter or a very thin filter) to measure Hp(0.07), and the other part of the holder may have a thicker filter that allows for measurement of Hp(3) or Hp(10). The thicker filter or filters shield the low‑energy photons and beta radiation, and allow only the more penetrating radiation to deposit energy. Some dosimeters have multiple filters of different thicknesses and compositions that allow them to discriminate among different energy levels.
Active dosimeters most commonly used to measure photon and beta radiation display dose readings electronically on a screen. Pencil dosimeters (also known as pocket dosimeters) are also active dosimeters. In a pencil dosimeter, doses are indicated by the position of a thin line on a radiation exposure scale.
There are many dosimeter technologies available for measuring photon and beta radiation. Passive whole-body dosimeters include thermoluminescent dosimeters and optically stimulated luminescence dosimeters. Active whole-body dosimeters include direct-reading dosimeters, also known as electronic personal dosimeters or personal alarming dosimeters.
Measurement techniques for determining doses resulting from photon and beta radiation are generally inappropriate for measuring neutron radiation since neutrons interact differently in matter.
Various neutron dosimeter options exist. Examples include personal neutron dosimeters (of which the most popular is the solid-state nuclear track detector) and portable neutron survey meters. These dosimeter technologies are further described in section 4.1.
Many factors influence the quality of a dosimeter’s results:
- A dosimeter’s response will vary depending on the energy of the radiation and the angle of incidence of radiation relative to the dosimeter’s detector.
- Dosimeters vary in their ability to detect different types of radiation (photon, beta or neutron).
- A dosimeter’s signal can fade over time; this can be caused by environmental factors such as temperature, light and humidity.
- Some dosimeters are limited in their ability to perform in pulsed radiation fields. Footnote 2
- Some dosimeters are more sensitive and can detect a lower quantity of radiation than others.
- Dosimeters differ in their ability to withstand severe environmental conditions.
Any limitations regarding the above factors should be discussed with the dosimetry service provider or manufacturer so that they are well understood. These limitations should be documented and workers should be trained so that appropriate precautions can be taken to prevent any impact on dose results. For example, many active dosimeters are known to perform poorly in pulsed radiation fields. Therefore, if pulsed radiation fields contribute significantly to dose, this should be taken into account when selecting the most appropriate dosimeter for ascertaining worker dose.
A dosimeter’s response is the measured or evaluated value divided by the conventionally true value. The conventionally true value, also known as “best estimate,” is the value attributed to a quantity and accepted as having an uncertainty appropriate for a given purpose. The response will vary depending on the type and energy of radiation to which the dosimeter is exposed. Dosimetry service providers may provide the option to apply standard correction factors applicable to specific radionuclides or energies to obtain more accurate results. These options should be carefully considered in consultation with the dosimetry service provider. If correction factors are applied, they should be documented and reviewed if any changes occur in the workplace or work activities that could affect their validity.
Dosimeters should be secured to the body to prevent them from falling off during work activities, facing outward and not covered by other items or devices. They should be worn on the trunk of the body between the waist and shoulders at the location of the highest expected exposure (or placed as per the manufacturer’s specifications).
When dosimeters are not worn, they should be stored in an area where dose rates are as close to background as possible and where storage conditions are favourable (areas where dosimeters are protected from direct sunlight, extreme temperature conditions, dust, etc.). Dosimeters should never be stored near radioactive materials or exposure devices. At least one representative control dosimeter of the same type should be kept in each dosimeter storage area during the wearing period. The control dosimeter is used to monitor non-occupational dose, to which personal dosimeters are also exposed while they are not worn (i.e., during storage and transport). This includes dose from background radiation and other sources that are not related to licensed activities. When processed, the doses reported by the control dosimeter may be subtracted from the doses reported by worker dosimeters so that the net occupational dose can be accurately determined. Control dosimeters should be shipped with dosimeters during transport in order to identify potential exposure to radiation during transport. Dosimeters should be shipped using services that will not result in inadvertent exposure to radiation above ambient background levels while the dosimeters are in transit. For example, shipping services that ship radioactive material should not be used.
During air travel, the dosimeter should not be packed in checked or carry-on baggage. This will prevent a non-personal dose from being recorded on the dosimeter as a result of exposure to X‑ray/CT scanners in use by most airports as part of baggage security screening protocols. Best practice is to carry or wear the dosimeter through the security screening point.
Precautions should be taken to protect dosimeters from being contaminated with radioactive material. However, this should always be done in consultation with the manufacturer or dosimetry service provider to ensure that any precautions taken do not impact dosimeter results.
Procedures should be in place to deal with dosimeters that have been compromised (e.g., lost, damaged or subjected to non-personal exposures). These situations should be investigated and appropriate actions should be taken as soon as possible. The investigation should involve discussions with the worker whose dosimeter was compromised and with the dosimetry service provider. A replacement dosimeter should be provided and, if appropriate, a dose change request should be submitted to the CNSC as per guidance provided in Part C of this document.
4.1 Dosimeter technologies
The dosimeter technologies described in this section are examples of commonly used active and passive dosimeters. Other technologies are also available.
If a dosimeter reports an unexpected result or exceeds an action level, an investigation should be carried out as per REGDOC-2.7.1 [1]. This should include inspection of the dosimeter for contamination, if applicable. The dosimetry service provider should be consulted to investigate the analysis associated with the dosimeter in question.
4.1.1 Thermoluminescent and optically stimulated luminescence dosimeters
Thermoluminescent dosimeters (TLDs) are commonly used dosimeters. Once a TLD has been read, it cannot be reread to verify the result.
There are many types of TLDs available, including lithium fluoride, calcium sulfate and lithium borate dosimeters.
An optically stimulated luminescence dosimeter (OSLD) offers advantages that include the ability to be reread, and it has a low minimum measurable dose. OSLDs operate much like TLDs, the major difference being that light, rather than heat, provides the energy required to return the excited electrons to their ground state, producing luminescence proportional to the absorbed dose.
4.1.2 Direct-reading dosimeters
Direct-reading dosimeters (DRDs) are active dosimeters, since they display doses and dose rates while in use. Many DRDs have alarms that sound at pre-set doses and dose rates. The most commonly used DRDs display dose readings electronically and are composed of either a diode or a Geiger-Müller (GM) detector. However, ion chamber pencil dosimeters are still used as well.
DRDs are used for controlling exposure and are often worn in addition to a passive dosimeter. When there is a possibility that radiation fields could increase unexpectedly by a factor of 10 or more, a DRD should be used. For many years, DRDs have been used as dose control devices, particularly in the nuclear power industry and for industrial radiography.
DRDs are not typically used to measure doses of record but may be used for this purpose when licensed dosimetry is not required or in the event of a lost or damaged passive dosimeter. When active dosimeters are used, the energy range, sensitivity, linearity and precision should be appropriate for the exposure situations in which they will be used. In addition, quality control measures and calibration procedures should be in place to ensure that dosimeters are performing appropriately. In particular, if active dosimeters using GM tubes as detectors are used, their potentially significant under-response to high-dose-rate fields (>100 mSv/h) should be taken into consideration.
4.1.3 Solid-state nuclear track detector
A solid-state nuclear track detector uses a plastic material called CR-39 (composed of allyl diglycol carbonate). CR-39 technology is based on the reaction of neutrons with material in the detector. The reaction produces charged particles, such as protons, at the site of interaction. The protons produce tracks in the dosimeter that are made visible through a chemical etching process. After etching, the tracks are counted to determine the dose.
4.1.4 Portable neutron survey meters
Portable neutron survey meters are based on a design that allows them to respond to neutrons with a wide range of energies. They are calibrated for a specific dose conversion coefficient, which can vary over more than 2 orders of magnitude. Therefore, the neutron energies should be well known for neutron survey meters or set for a conservative value of dose conversion rate. When used, portable neutron survey meters are usually placed in an area in the work environment where radiation readings are highest. By integrating the dose rate over the period of time that workers spend in that location, doses can be estimated and assigned to each worker. With this measurement method, the neutron survey meter’s highest measured dose rate is used. This ensures that resulting assigned doses remain conservative.
4.2 Whole-body dosimetry
The most common dosimeters are those used to ascertain external effective dose to the whole body and/or equivalent dose to the skin of the whole body as a result of external exposure to photon and beta radiation. These dosimeters are commonly referred to as “whole-body dosimeters” or “whole-body badges” and are typically worn on the front of the torso between the waist and neck. Whole-body dosimeters typically measure the deep dose to the whole body using Hp(10), and Hp(0.07) for shallow (skin) dose to the whole body in uniform exposure situations. The most common dosimeter technologies used as whole-body dosimeters include TLDs, OSLDs, and DRDs.
In some situations, the use of multiple whole-body dosimeters (commonly known as “multiple badging”) is more appropriate to ascertain external effective dose than the use of 1 whole-body dosimeter worn on the trunk. These situations arise when worker exposures to radiation are non‑uniform.
4.3 Multiple whole-body dosimetry
The guidance provided in this section on the use of multiple whole-body dosimeters is based on the American National Standards Institute/Health Physics Society publication ANSI/HPS N13.41-2011 (R2018), Criteria for Performing Multiple Dosimetry [6].
The following are situations in which radiation exposures are non-uniform and may require the use of multiple whole-body dosimeters.
-
Workers wear protective clothing or partial body shields, as in the following examples:
- lead aprons worn to offer protection to a worker who is required to be in a diagnostic imaging room at the time of an exposure
- partial body shields used in nuclear substance laboratories, where bench-top shielding is used to protect workers who are preparing radiopharmaceuticals
-
Workers are required to maintain a fairly constant position with respect to a localized field, as in the
following examples:
- boiler maintenance work in a nuclear generating station, where the upper part of the body may be exposed to higher levels of radiation than the lower part
- work performed in close proximity to a localized source of radiation, so that the parts of the body closest to the source are in a more intense field than the rest of the body
- Operations are performed near radiation leaks, such as cracks or small holes in shielding materials.
- Workers are exposed on the sides of the body opposite to where the dosimeter is usually worn – for example, maintenance work that requires diving into used nuclear fuel bays, where there is a potential for exposure to high dose rates from multiple angles.
Section 4.3.1 provides guidance for the first 3 situations above.
For the fourth situation listed above, the number of dosimeters required would be determined on a case-by-case basis: 1 dosimeter should be worn at the usual wearing location, and additional dosimeters should be worn at other exposed areas of the body. The external effective dose would be calculated using an algorithm determined to be appropriate for the specific exposure situation. An assessment should be performed on a case-by-case basis to determine the appropriate algorithm.
While multiple whole-body dosimeters may be used at any time to provide more accurate dose estimates, the use of more than 1 dosimeter is strongly recommended when the following 2 conditions exist:
- The personal dose equivalent to any portion of the body (such as the head) has the potential to vary by 50% from the personal dose equivalent that would be measured with the dosimeter in its usual wearing location (the trunk).
- The resulting personal dose equivalent could exceed 10% of a dose limit when a significant component of the effective dose from external sources comes from a non-uniform radiation field.
When it has been determined that a worker will carry out specific tasks wearing multiple whole‑body dosimeters, in addition to routine work in a uniform field where routine monitoring is used, a special set of dosimeters should be issued to the worker to be worn during the specific work instead of routine monitoring dosimeters. The worker’s total dose is the sum of the dose associated with work in the uniform radiation field where routine monitoring is used and the dose(s) for 1 or more periods of work in a non-uniform field where multiple dosimeters are used.
The placement of multiple dosimeters should be clearly documented. A dosimeter worn on a part of the body covered by a lead apron should be worn between the lead apron and the body.
The number of dosimeters needed when using multiple dosimeters depends on the radiation field, the work to be performed, the location of the worker relative to the source(s) of radiation and the level of information desired from multiple dosimetry.
4.3.1 Calculating whole-body external effective dose from multiple dosimeters
To obtain an estimate of the external effective dose, E, the doses reported by multiple dosimeters may be combined using a weighted sum. To this end, the body is considered to be made up of compartments, and each compartment is monitored by an assigned dosimeter.
Compartment factors (WC) have been developed for various compartments or areas of the body. The compartments and the associated compartment factors presented in table 2 are based on ICRP Publication 103 [4] tissue weighting factors that account for the radiosensitivities of tissues and organs that make up various compartments.
| Compartment | Compartment factor, WC |
|---|---|
| Head and neck | 0.12 |
| Thorax, above the diaphragm | 0.40 |
| Abdomen, including the pelvis | 0.46 |
| Upper right arm, including the elbow | 0.005 |
| Upper left arm, including the elbow | 0.005 |
| Right thigh, including the knee | 0.005 |
| Left thigh, including the knee | 0.005 |
The dose equivalent, Hp(10), for each compartment may be determined by the results of the dosimeter worn at that location of the body. If there is no dosimeter placed on a compartment area, the dose equivalent determined by a dosimeter placed on a nearby part of the body that is shielded in the same way could be used.
The external component of the whole-body effective dose, E, can be calculated using the following equation:
(1)
Where:
| WC = | the compartment factor | (unit-less) |
|---|---|---|
| Hp,C = | the dose equivalent assigned to compartment C | mSv |
If a need for a more complex method of combining dosimeter results arises, further guidance is provided in ANSI/HPS N13.41-2011 (R2018), Criteria for Performing Multiple Dosimetry [6]. For example, in some situations, neck collars (also known as thyroid collars) are worn along with the lead apron. In this case, the model may be adjusted, as the neck is protected by the collar.
Example calculation
When protective lead aprons are used, at least 2 dosimeters should be worn (1 on the thorax and 1 on the head or neck). An example calculation is provided below for the common situation in which workers wear protective lead aprons covering the thorax, abdomen and thighs. In this example, workers wear 1 dosimeter on the head or neck facing the source of radiation and 1 dosimeter on the trunk under the apron facing the source of radiation. The head/neck dosimeter measures the personal dose equivalent to the head and neck and the unshielded arms. The trunk dosimeter worn under the apron measures the personal dose equivalent to the thorax, abdomen and thighs. Table 3 provides an example of a calculation of the external component of the effective dose for each compartment.
| Compartment | Compartment factor, WC | Assigned dosimeter | Personal dose equivalent, Hp,C (mSv) | Compartment effective dose, EC (mSv) |
|---|---|---|---|---|
| Head and neck | 0.12 | Head/neck | 5.0 | 0.6 |
| Thorax, above the diaphragm | 0.40 | Trunk | 0.2 | 0.08 |
| Abdomen, including the pelvis | 0.46 | Trunk | 0.2 | 0.092 |
| Upper right arm, including the elbow | 0.005 | Head/neck | 5.0 | 0.025 |
| Upper left arm, including the elbow | 0.005 | Head/neck | 5.0 | 0.025 |
| Right thigh, including the knee | 0.005 | Trunk | 0.2 | 0.001 |
| Left thigh, including the knee | 0.005 | Trunk | 0.2 | 0.001 |
Therefore, summing the effective dose for each compartment, whole-body external effective dose is 0.82 mSv.
4.4 Extremity dosimetry
The RPR require that licensed dosimetry be used to monitor doses of radiation received by and committed to NEWs who have a reasonable probability of receiving an equivalent dose to the skin, or to the hands and feet, that is greater than 50 mSv in a 1-year dosimetry period. Hands and feet are also referred to as the extremities. ANSI/HPS N13.41-2011 (R2018), Criteria for Performing Multiple Dosimetry [6], defines the hand as the arm below the elbow and the foot as the leg below the knee. The operational quantity Hp(0.07) is commonly used to measure doses to the skin, and to the hands and feet.
Since the equivalent dose limit for the hands and feet is set based on preventing a tissue reaction, the dose limit applies to each individual hand and foot. Therefore, when assessing the dose to the skin of the left hand and the right hand, or to the left foot and the right foot, they are treated as separate entities, with separate equivalent dose limits, and doses to different extremities should be recorded separately.
Extremity dosimeters are used to measure Hp(0.07) and should be worn on or as close as practicable to the 1 cm2 area of the extremity that receives the highest dose. It is also common practice to wear extremity dosimeters on both hands. Monitoring is most commonly done with TLD rings for the fingers or TLD chips taped or strapped to the extremities. In some cases, a whole-body dosimeter is worn on the wrist or ankle with the use of a strap. The wearing instructions of the dosimetry service provider should be followed. In general, the extremity dosimeter should be worn next to the skin, inside any clothing that shields the skin from exposure to low-energy photons and beta radiation. Placing the dosimeter under the clothing also protects it from potential contamination.
A worker who handles radioactive sources by hand may need to wear extremity dosimeters in order to adequately measure the equivalent dose to the hands. Nuclear medicine and nuclear fuel processing are 2 examples of industry sectors whose workers wear extremity dosimeters. In these situations, the administration of nuclear substances or the processing of nuclear fuel could expose the worker’s hands to higher levels of radiation than the rest of the body. Nuclear power plant workers also wear extremity dosimeters when their duties cause their hands or feet to come in close contact with nuclear substances.
4.5 Lens of the eye dosimetry
A workplace hazard assessment should be carried out and documented to evaluate if workers are at higher risk of receiving elevated exposure to the lens of the eye. If it is determined that workers are at higher risk, doses to the lens of the eye should be estimated. These situations include:
- workers subject to non-uniform exposures to the eye
- workers exposed to weakly penetrating radiation that contributes to dose to the lens of the eye, but less so, or not at all, to the effective dose (i.e., whole-body dose)
Radiological workplace hazards should be reviewed and evaluated to determine if additional measures should be put in place to better protect workers from radiation exposure to the lens of the eye. In some cases, doses to the lens of the eye may be effectively reduced through:
- implementation of engineered controls that, ideally, should be considered at the design stage of facilities and equipment
- use of personal protective equipment, such as protective eyewear
- use of administrative controls, such as procedural requirements and restrictions
The workplace hazard assessment should determine if any workers fall into 1 of the following 2 categories:
- workers exposed to weakly penetrating radiation, such as beta particles or photons of low energies (i.e., below about 40 keV) – note that beta radiation requires a maximum energy greater than 700 keV to penetrate to the sensitive depth of the lens; therefore, beta energies below 700 keV need not be considered
-
workers exposed to non-uniform radiation fields, including when:
- the head is closer to the radiation source than the rest of the body (such as when viewing or manipulating a radioactive source – for example, looking closely at a syringe containing medical isotopes or inspecting manufactured fuel pellets)
- the trunk of the body is shielded (e.g., by equipment or protective gear) and the eyes are not
If workers fall into 1 or more of the above 2 categories, the nature of the exposures should be documented and the method(s) of assessing doses to the lens of the eye should be determined. Individual monitoring for the lens of the eye includes:
- dosimeters worn near the lens of the eye that measure Hp(3)
- dosimeters worn near the eyes or on other parts of the body that measure Hp(10) or Hp(0.07)
If workers do not fall into 1 of the 2 categories, doses to the lens of the eye can be assumed to be equivalent to Hp(10) or Hp(0.07), and doses may be determined through measurements by whole‑body dosimeters worn on the trunk. Using this assumption, compliance with effective dose limits will also ensure compliance with the equivalent dose limits for the lens of the eye.
Tables A.1 and A.2 in appendix A provide specific guidance on how to choose the appropriate dosimeter for various situations. This guidance is based on information from International Atomic Energy Agency (IAEA) TECDOC‑1731, Implications for Occupational Radiation Protection of the New Dose Limit for the Lens of the Eye [7]. Please refer to that document for further information.
To determine whether monitoring the lens of the eye for neutron exposure is required, the workplace hazard assessment should identify workers exposed to neutron radiation. This assessment should also evaluate the neutron contribution to the total eye dose. When exposures are non-uniform in neutron fields and where the eyes are preferentially exposed, personal dosimeters that measure Hp(10) and that are worn near the eyes may provide a conservative estimate of the neutron dose to the lens of the eye in some circumstances. Note that this is in addition to neutron dosimetry used to monitor dose to the whole body (as described in section 4.6).
The dosimeter selected to measure Hp(3) should have the appropriate filter to measure the dose equivalent at a depth of 3 mm. Dosimeters should also be capable of measuring a range of doses appropriate for potential worker doses and be appropriate for workplace radiation fields. Dosimetry service providers should be consulted to ensure dosimeters are appropriate for the workplace environment in which they may be used. A dosimetry service provider that has a management system and calibration procedure should be selected.
When a dosimeter is worn near the eyes to monitor dose to the lens of the eye, the location where it should be worn (e.g., left side of the left eye, right side of the right eye, centre of the forehead) should be assessed. The location where the dosimeter would receive the highest dose should determine the placement of the dosimeter.
Eye shielding with lead may be used to reduce dose rates from photon radiation. Non-leaded plastic eye shielding is not effective for shielding photon radiation but may reduce dose rates from beta radiation. If eye shielding is used, the dosimeter should be placed in such a way as to account for the shielding. This means that the dosimeter should be located between any shielding material and the lens of the eye. If this is not practicable, a filter that mimics the shielding may be used with the dosimeter or correction factors may be applied. The basis for any correction factors used should be documented.
4.6 Neutron dosimetry
Many factors (such as the nature of the source; the thickness, shape and composition of shielding material; or the geometry of the work environment) can alter the neutron energy spectrum that comes into contact with a worker’s body. This makes neutron dosimetry very challenging.
Doses to workers from exposures to neutrons may be ascertained using active or passive monitors.
Passive neutron monitors (including, but not limited to, CR-39 dosimeters) should be used where feasible. They should be appropriate for the neutron energy spectrum at the workplace. More than one type of neutron dosimeter should be used to monitor workers exposed to neutron energy spectra that are broader than that for which a single type of neutron dosimeter has been calibrated.
Personal neutron dosimeters are used to measure Hp(10) and should be worn on the trunk of the body between the waist and neck at the location of the highest expected exposure. As described in section 4.5, when exposures are non-uniform in neutron fields and where the eyes are preferentially exposed, personal dosimeters that measure Hp(10) from neutron radiation may be worn near the eyes to provide a conservative estimate of neutron dose to the lens of the eye in some circumstances.
Active neutron monitors consist of portable neutron monitoring instruments. Such instruments may be used to characterize the neutron fields in a workplace. Personal neutron doses may be derived from the results of such workplace characterizations and known personnel occupancy times. When used to characterize neutron fields in a workplace, portable monitoring instruments should be placed in the locations where the potential for neutron exposures exists. In addition, the neutron energy spectra at the workplace should be known in order to choose an appropriate monitoring instrument. In cases where the neutron energy spectrum at a given location is very broad, more than one type of device may be needed.
Portable neutron monitoring instruments should be used for dosimetry purposes only when they are the most feasible option for ascertaining doses to workers from neutron radiation.
Portable neutron monitoring instruments should not be used in work areas in which there are spatial variations in neutron dose rates such that the instrument may not reflect doses to workers. If portable neutron monitoring instruments are used for dosimetry, licensees should demonstrate that there is no appreciable spatial variation in dose rates, so that the monitoring results are representative of worker exposures.
5. Ascertaining External Dose Through Estimation
Although direct monitoring is the preferred method for ascertaining external doses to workers, paragraph 5(2)(b) of the RPR states that “if the time and resources required for direct measurement as a result of monitoring outweigh the usefulness of ascertaining the amount of exposure and doses using that method,” doses may be ascertained through estimation. For the purpose of this document, estimation refers to 2 types of approaches to estimating doses: indirect (i.e., workplace) monitoring and dose modelling (i.e., calculating doses based on the characteristics of the source, exposure geometry and other relevant parameters). This section provides guidance on indirect monitoring and dose modelling. Guidance is also included on how to evaluate the equivalent dose to the skin as a result of a skin contamination incident. Quality assurance measures that should be considered when ascertaining doses using dose estimation methods are also included.
5.1 Indirect monitoring
Indirect or workplace monitoring consists of measuring the dose rate in a radiation field and multiplying this dose rate by each worker’s occupancy time in that field. Workplace monitoring provides information on dose rates in a workplace and can help with work planning and exposure control. It may be used for prospective assessments of doses as a planning tool. It can also be used for retrospective assessments of doses, such as in situations in which doses are low and constant over time.
For the purpose of estimating personal doses, workplace measurements should only be used in radiation fields that are uniform and consistent over time. The locations of workplace monitoring should be representative of worker occupancy. If the radiation field is uniform in space and in time, only a few monitoring locations need to be used. Locations where indirect monitoring is carried out should be assessed to determine where instruments should be placed and how many instruments should be used. The number of workplace measurement locations should be increased for radiation fields that are non-uniform in space. Measurements should be taken immediately following environment changes that have the potential to affect monitoring results. If changes are frequent or sudden, monitoring should be continuous. When ascertaining doses on the basis of workplace monitoring, the monitoring results should be representative of all working areas where doses are ascertained in this manner. Workplace monitoring data, including the time and location of each measurement and the associated result, should be documented.
Workplace monitoring to estimate personal doses should utilize the appropriate instrumentation. For mixed radiation fields, it may be necessary to use more than one type of instrument. In order to ensure workplace monitoring is appropriate, the instrument(s) used should be:
- selected to measure the types and energies of radiation present
- selected to cover the range of dose rates present
- selected to operate under environmental conditions or external influences present
- calibrated appropriately for the type and energies of radiation present
- placed in an appropriate location and direction such that measurements conservatively reflect worker doses
- capable of scalar counting if very low doses are to be measured
Instruments should also be selected so that it is obvious to the individual taking measurements when the instrument is beyond its range.
Instruments used to estimate personal doses typically measure in operational quantities, such as H*(10) and/or H’(0.07, Ω). An explanation of operational quantities can be found in section 3. It is important to determine which operational quantity is appropriate to use as a surrogate for the protection quantity of interest. For more information, consult ICRU Report 51, Quantities and Units in Radiation Protection Dosimetry [5]. For example, the ambient dose equivalent, H*(10), may be used as a surrogate for effective dose. For exposures to low-penetrating radiation, either the ambient dose equivalent H*(0.07) or the directional dose equivalent H’(0.07, 0º) may be used as a surrogate for equivalent dose to the skin.
5.1.1 Special consideration for the lens of the eye
Direct monitoring is the preferred method for assessing dose to the lens of the eye. However, when radiation fields are predictable over long periods of time, it is possible to estimate doses using indirect monitoring at relevant locations. The locations should be representative of the conditions under which individuals will be exposed. If ambient monitoring is being considered, then instruments that measure ambient dose equivalent and directional dose equivalent may be used. If ambient monitoring is being considered, Hp(10) and Hp(0.07) may be replaced with H*(10) and H’(0.07) respectively, in table A.1 of appendix A, which provides guidance on direct monitoring.
5.2 Dose modelling
Dose modelling to ascertain external doses to workers involves calculating doses based on knowledge of the exposure scenario, such as the source term, the exposure geometries and the exposure times, and using published dose coefficients and shielding information. Various software packages are available either online or for purchase that allow the user to calculate doses and dose rates from various types of sources and geometries.
Dose modelling to ascertain doses to workers may be used when the characteristics of the sources present in the work environment and the exposure geometries are well understood.
Dose modelling methods to ascertain worker doses should be consistent with the following quality practices.
- Dose modelling should be carried out only by trained and qualified workers.
-
Procedures for modelling doses should:
- be in place to document all work activities that can influence the assignment of the correct dose to the right individual and the maintenance of a dose record system
- provide details of dose modelling methods
- be reviewed and revised as needed when changes in the workplace may impact the precision, accuracy and reliability of dose estimates
- Verification of dose modelling methods and results should be carried out by trained and qualified persons other than those who have participated in the work being verified.
For more guidance on carrying out simple dose or dose-rate calculations, refer to the CNSC’s Radionuclide Information Booklet [8].
5.3 Skin contamination
This section provides guidance to licensees on evaluating skin dose as a result of a skin contamination incident.
Experience has shown that most skin contamination incidents, if detected promptly, actually result in relatively low equivalent doses. The general principles for responding to skin contamination incidents are as follows:
- The circumstances of the event are documented, recorded and investigated to ensure that work practices are optimized, and to minimize the probability of repeat occurrences.
- A skin dose is calculated and recorded by the licensee.
- The licensee reports the incident to the CNSC in accordance with its licence requirements, as applicable.
5.3.1 Contamination meter efficiencies
Guidance on monitoring for radioactive contamination is provided in appendix C of REGDOC‑2.7.1 [1]. This guidance should be used to establish detector efficiencies for radionuclides used before unsealed sources are manipulated, even if skin contamination is unlikely.
5.3.2 Background measurements
Background count rate measurements using the selected contamination meter should be made and kept on record for future use in case of a skin contamination incident. These measurements should be made in a low-dose-rate area where nuclear substances are not present.
5.3.3 Measuring skin contamination
Step-by-step instructions are provided below to measure and record the net count rate.
- Estimate the size of the contaminated skin area using the contamination meter.
-
Measure and record the count rate directly over the affected portion of skin with the highest count rate, and record the time of measurement as well as the time of the contamination event.
If practicable, and if a radiation detector is within close proximity, the first measurement should be taken before decontamination efforts.
The measurement should be taken with the detector placed at a known distance as close to the skin as possible (e.g., 0.5 cm) without direct contact.
-
Determine the net count rate in counts per second (cps) by subtracting the background count rate from the count rate measured on the skin. If the net count rate is in counts per minute, divide it by 60 to convert it to counts per second.
If the net count rate is above zero, decontaminate by washing immediately with lukewarm water. However, excessive cleaning should be avoided to prevent damaging the skin and causing an intake by absorption through the skin.
Repeat steps 1 through 3 until the net count rate is zero or until subsequent measurements are no longer decreasing.
Some situations may warrant an attempt to extract fixed-skin contamination more quickly, such as by wearing an impermeable glove over the affected skin surface to encourage sweating. The radiation safety officer or equivalent radiation protection authority should be consulted for specific guidance.
5.3.4 Calculating skin dose from contamination
If the timing of the skin contamination event is not known, or if a significant amount of time (more than 30 minutes) has elapsed between the contamination event and the first measurement, a conservative assumption with respect to the time of the event should be made. For example, the time of contamination may be assumed to be the time the radioactive material was first handled.
The average surface concentration (Bq/cm2) for each measurement may be determined using the following formula:
(2)
Where:
| = | the average surface concentration in Bq/cm2. If the instrument reports its results in Bq/cm2, it is important to understand the surface area that was assumed for the conversion because a correction factor may be required. For example, if an instrument reports a result in Bq/cm2 based on a 100 cm2 calibration source and the contaminated skin surface area is 1 cm2, the result reported by the instrument should be multiplied by a factor of 100. |
|---|---|
| Net count rate = | the measured average count rate minus the background count rate in counts per second (if the net count rate is obtained in counts per minute, divide the measurement by 60 to obtain the value in counts per second). |
| Area = | the contaminated skin surface area in cm2 if the contaminated area is less than the probe surface area and the measurement was taken such that the area of contaminated skin was directly under the probe (if the area is unknown or the skin is unevenly contaminated, 1 cm2 may be conservatively assumed), or the probe’s active surface area in cm2 if skin is evenly contaminated over a larger area than the probe |
| ε = | contamination meter efficiency in cps/Bq |
The following formula may be used to calculate the skin dose in µSv, corresponding to each measurement interval:
(3)
Where:
| DCF = | skin dose rate conversion factors in µSv/h per Bq/cm2 (see table 4 below) |
|---|---|
| T1/2 = | half-life in hours |
| T = |
time elapsed, in hours For the first measurement, T is the elapsed time between the first and second measurement plus the estimated elapsed time between the contamination event and the first measurement. For subsequent measurements, T is the elapsed time between the current and subsequent measurement. |
Table 4 is adapted from IAEA-TECDOC-1162, Generic Procedures for Assessment and Response During a Radiological Emergency [9], and presents equivalent dose rate conversion factors that should be used when applying equation 3. Licensees may propose alternative DCF values for review by CNSC staff.
| Radionuclide | Half-life (hours) | Conversion factors (µSv/h per Bq/cm2) |
|---|---|---|
| 14C | 5.02 x 107 | 0.32 |
| 18F | 1.83 | 1.9 |
| 32P | 343 | 1.9 |
| 67Ga | 78.2 | 0.35 |
| 90Sr/90Y | 2.55 x 105 | 3.5 |
| 90Y | 64.1 | 2.0 |
| 99Mo/99mTc | 65.94 | 1.9 |
| 99mTc | 6.0 | 0.25 |
| 111In | 67.2 | 0.38 |
| 123I | 13.2 | 0.38 |
| 125I | 1,442 | 0.021 |
| 131I | 192 | 1.6 |
| 201Tl | 73.0 | 0.27 |
A list of conversion factors for additional radionuclides may be found in IAEA-TECDOC-1162 [9] and in the Health Physics article titled “Electron Dose-Rate Conversion Factors for External Exposure of the Skin from Uniformly Deposited Activity on the Body Surface” [10].
If the final net count rate is zero, sum the calculated doses to obtain the total skin dose. However, if the net count rate is not zero, determine the dose for the time following the last measurement using the formula below and then sum the doses to obtain the total skin dose:
(4)
Skin thicknesses may be taken into account to refine the skin dose estimates from skin contamination events; this will be assessed by the CNSC on a case-by-case basis.
Part B – Internal Exposure
6. Quantities
Internal exposures are those exposures to ionizing radiation that result from radionuclides that have been taken into the body. Quantities that are specific to ascertaining doses from internal exposure are described in this section.
The committed equivalent dose, HT(50), is the equivalent dose received by an organ or tissue from a radionuclide during the 50 years after the radionuclide is taken into the body of a person 18 years of age or older. Footnote 3
The committed effective dose (CED), E(50), is the effective dose from a radionuclide during the 50 years after the radionuclide is taken into the body of a person 18 years of age or older. Footnote 4
The annual limit on intake (ALI) is the activity of a radionuclide that, when taken into the body, will deliver a CED of 20 mSv. ALI values may be calculated for inhalation or for ingestion. The ALI for inhalation (ALIinh) is given by
(5)
The ALI for ingestion (ALIing) is given by:
(6)
In the above equations, the dose coefficients einh(50) and eing(50) are the CED per unit intake by inhalation and ingestion, respectively. These values should be based on ICRP default values applicable to the exposure scenario, when site-specific characteristics of the nuclear substances of interest (e.g., solubility, particle size) are not known. For inhalation intakes of particulates, unless site-specific information is available, the particle size (activity median aerodynamic diameter, or AMAD) may be assumed to be 5 μm. For inhalation intakes of gases and vapours, unless site‑specific information is available, the appropriate CED per unit intake should be selected according to ICRP recommendations. ICRP default dose coefficients for inhalation or ingestion should be adopted from ICRP Publication 119 [11].
The derived air concentration (DAC) is the concentration of a radionuclide in air that, when inhaled at a breathing rate of 1.1 m3 per hour for 2,000 working hours per year, results in the intake of 1 ALI of that radionuclide.
The DAC for a radionuclide is given by:
(7)
7. Intake Monitoring Methods
Monitoring workers for potential intakes of radionuclides may be conducted through either individual measurement methods or workplace measurements.
7.1 Individual monitoring
The purpose of individual intake monitoring is to verify and document that workers are adequately protected from internal radiological risks and to demonstrate compliance with the RPR. More specifically, individual intake monitoring aims to ascertain workers’ doses, serve as an indicator of potential intake and, overall, support the licensee’s radiation protection program. In emergency situations, the purpose of individual intake monitoring is to ascertain and document workers’ doses, including the absorbed dose to organs or tissues, and to serve as a trigger for initiating health surveillance and treatment.
Monitoring for intakes of radionuclides may consist of both workplace and individual monitoring. The types of workplace and individual monitoring methods at a facility (or location where a licensed activity is being carried out) should be selected to ensure the detection of those radionuclides identified by the radiological characterization for the facility or licensed activity that have the potential to be taken into the body in normal and abnormal (unplanned) operating conditions (e.g., as a result of the re-suspension of loose surface contamination or the inhalation of airborne radioactivity). The intake monitoring program is considered an integral part of the radiation protection program and should provide the necessary data to ascertain the dose to workers from intakes of radionuclides or trigger the ascertainment of worker doses in a timely manner.
Individual monitoring may consist of measuring radionuclide activity in the body (known as either in vivo monitoring or in vivo bioassay; the terms are equivalent), monitoring excreta (known as either in vitro monitoring or in vitro bioassay), taking air samples with personal air samplers, or a combination of these methods. The preferred monitoring method depends on a number of factors, which are discussed in this section.
In vivo monitoring involves photon (e.g., gamma radiation) detectors placed at specific positions relative to the person being measured in order to detect photons emitted by radionuclides that have been deposited within the person’s body. This method can be used only for radionuclides that emit X‑ray or gamma radiation, radionuclides that emit positrons (via the detection of annihilation gamma radiation) or radionuclides that emit energetic beta particles. In the latter case, bremsstrahlung radiation is detected. In vivo monitoring is not the method of choice when the radionuclides to be detected emit gamma or X‑ray radiation with a low yield, when they do not emit radiation that can readily be detected outside the body (e.g., photons of energy less than 25 keV) or when their biological half-time or physical half-life is short (e.g., less than 1 day). For further information, consult ICRU Report 69, Direct Determination of the Body Content of Radionuclides [12].
In vivo monitoring methods include whole-body monitoring and partial-body monitoring. Whole‑body monitoring should be used to monitor for intakes of radionuclides that are rapidly absorbed from the respiratory tract into systemic circulation, and that either distribute uniformly throughout the body, as is the case for Cs-134 for example, or distribute throughout several organs, such as Fe-59. Partial-body monitoring of the relevant organ should be selected to monitor for radionuclides that are preferentially deposited in one organ. These include, for example, I-131, for which thyroid monitoring is appropriate. In addition, lung monitoring is recommended for radionuclides that are absorbed slowly from the respiratory tract (i.e., materials with Type M or S absorption Footnote 5 ). According to ICRP Publication 119, Compendium of Dose Coefficients Based on ICRP Publication 60 [11], such radionuclides include U-235 and Am-241.
In vivo measurements are acceptable for detecting photon-emitting radionuclides embedded in a wound. Further guidance on intakes via wounds is presented in section 12.
Detailed guidance on establishing an in vivo measurement facility, including construction, installation and operation, is not within the scope of this document. It may be found, however, in IAEA Safety Series No. 114, Direct Methods for Measuring Radionuclides in the Human Body [14], and ICRU Report 69, Direct Determination of the Body Content of Radionuclides [12].
In vitro monitoring generally involves urinalysis, and may also include fecal bioassay in the case of inhaled insoluble compounds, as well as other investigative measurements such as nasal smears. Ideally, urine bioassay programs – with the exception of tritium bioassay – created for the purpose of dosimetry should be designed to collect and analyze samples gathered over a period of 24 consecutive hours. In many cases, this is not feasible or is not the most effective method of monitoring workers, in particular for routine monitoring programs. In such cases, alternatives may be acceptable. These may include:
- the collection and analysis of first-morning urine voiding
- the measurement of creatinine concentration in urine to estimate 24-hour excretion (based on a urine sample collected over part of a day)
-
normalization by:
- volume, with or without a correction for specific gravity
- the length of the sampling interval
The minimum quantity of urine required for the analysis of a sample depends on the analytical method. Licensees should document and implement a mechanism to (i) ensure that a sufficient quantity of sample is submitted in each in vitro sample submitted for analysis, and (ii) follow up with sample submitters to request a second sample when the sample is of insufficient quantity.
In vitro analyses involving radiochemical separation of radionuclides should include measures to control the measurement process by the use of chemical yield tracers. Such tracers may be added to samples to be analyzed or, alternatively, may be added to similar samples, such as artificial samples or samples from an uncontaminated subject. The licensee should establish acceptance criteria for in vitro sample results from the laboratory. Such criteria should include a minimum chemical yield. Samples with a chemical yield below this threshold should not be used for dosimetry, and a reanalysis of the sample should be requested.
In the case of urine bioassay measuring tritium excretion as tritiated water, single (spot) urine samples of a few millilitres (for routine monitoring) may be analyzed for tritium activity. Converting the concentration of tritiated water in urine to the resulting effective dose rate is addressed in appendix D.
Urine bioassay programs may also be useful for non-dosimetry purposes, specifically, as a screening tool to identify potential intakes of radionuclides. In such cases, spot samples may be sufficient to allow for the detection of intakes. However, the sample submission frequency and the sensitivity of the analytical method should be demonstrated to ensure that intakes potentially leading to an annual CED of 1 mSv do not go undetected. Urine bioassay programs should include measures to prevent contamination of the samples. Such programs should also ensure that the sample volume required for analysis is sufficient so that adequate sensitivity can be achieved to meet the needs of the radiation protection program it supports.
The analysis of fecal samples is generally carried out as part of a response to a known or suspected abnormal inhalation intake of Type M or S material. If possible, collection over a period of 2 to 3 days should occur in the first week following the abnormal intake. Fecal excretion rates of radionuclides in the first few days following an acute inhalation vary significantly. Furthermore, early fecal sampling results may allow for the identification of exposed individuals.
Nasal smears may be used as a screening tool to identify potential inhalation intakes. Positive nasal smear results should be followed up with in vitro and/or in vivo measurements, as appropriate for the radionuclide(s) identified and their associated solubility, in order to confirm whether an intake has occurred and to quantify it.
Several factors should be considered when selecting the method of bioassay monitoring. The first factor is the objective of monitoring – there should be a balance between the needs for intake monitoring and dose assessment. Intake monitoring requires timely information about the occurrence of intakes and should be based on the following indicators of intake, in order of preference:
- personal air sampler (PAS) or workplace static air sampler (SAS)
- nasal swabs
-
if appropriate for the radionuclides of concern:
- in vivo bioassay
- in vitro bioassay
When the objective of monitoring is ascertaining dose, the order of preference is different than above:
-
if appropriate for the radionuclides of concern:
- in vivo bioassay
- in vitro bioassay
- personal air sampling
Information on air sampling can be found in section 7.2. Table 5 illustrates suggested methods of bioassay measurement that may be performed for selected radionuclides, taking into account their physical and metabolic characteristics. Note that table 5 is not exhaustive and that the appropriate methods depend on the physical and chemical form of the radionuclide as well as its route of excretion.
| Bioassay method | Radionuclide | ||
|---|---|---|---|
| In vivo bioassay | |||
| Whole-body counting |
|
|
|
| Lung counting |
|
|
|
| Thyroid counting | 123I, 124I, 125I, 131I | ||
| In vitro bioassay | |||
| Liquid scintillation counting (β‑counting) of urine sample |
|
|
|
| Liquid scintillation counting (β‑counting) of urine sample after chemical separation |
|
|
|
| β‑counting of fecal sample after chemical separation | 14C (particulates) | ||
| Gamma spectroscopy of urine sample |
|
|
|
| Gamma spectroscopy of fecal sample (possibly after chemical separation) |
|
|
|
| Alpha spectroscopy of urine/fecal sample after radiochemical separation |
|
|
|
| Inductively coupled plasma mass spectrometry (ICP-MS) |
|
|
|
| Thermal ionization mass spectrometry (TIMS) | 239Pu, 240Pu | ||
* Measurement of bremsstrahlung radiation
** Alpha spectroscopy cannot normally distinguish between Pu-239 and Pu-240.
7.2 Types of individual intake monitoring programs and participant selection
Under paragraph 27(a) of the NSCA, every licensee is required to keep any records prescribed by the regulations under the NSCA, as well as a record of the dose received by or committed to each person who performs duties in connection with any activity that is authorized by the NSCA or who is present at a place where that activity is conducted. This is intended to apply to all persons who may be on the licensee’s premises and exposed to radiation, and who are therefore under the licensee’s responsibility with regard to determining and controlling doses. This requirement is also stated in subsection 5(1) of the RPR. A radiation exposure or dose can be ascertained by direct measurement as a result of monitoring, as required by paragraph 5(2)(a) of the RPR. Paragraph 5(2)(b) of the RPR stipulates that “if the time and resources required for direct measurement as a result of monitoring outweigh the usefulness of ascertaining the amount of exposure and doses using that method”, they are to be estimated.
Participation in an individual monitoring program should be based on workers’ likelihood of intakes during routine operations as well as during accidental situations. The monitoring program should be designed to provide sufficient data of a level of quality necessary to achieve the program’s objective in order to, for example, ascertain workers’ CED, assess the likelihood of an intake, and assess the potential for nephrotoxicity as a result of uranium intakes where applicable.
Sections 7.2.1 to 7.2.4 describe 4 types of individual monitoring programs:
- routine bioassay monitoring
- special bioassay monitoring
- confirmatory monitoring
- task-related monitoring
Baseline bioassay assessments are also described.
7.2.1 Routine bioassay monitoring
Routine monitoring is carried out in situations in which intakes of radionuclides by workers are probable during the normal operations of the licensed activity. It is also conducted to detect unplanned intakes, and is generally carried out when the potential for intakes is essentially continuous as a result of normal operations, that is, when intakes could occur at any time during normal operations. Because routine measurements are carried out at predetermined times, some assumptions are made about the time and pattern of intakes (e.g., acute vs. chronic, acute at the midpoint in the monitoring interval).
Routine monitoring programs should ensure that annual CEDs to workers of 1 mSv or more do not go undetected. The licensee should therefore identify which workers have a reasonable probability of receiving:
- an annual CED (i.e., resulting from all occupational intakes of radionuclides in 1 year) up to 1 mSv (for persons who are not NEWs)
- an annual CED greater than 1 mSv and a total annual effective dose (i.e., the sum of the annual effective dose from external sources and the annual CED) of up to 5 mSv (NEWs participating in a routine bioassay program that is not necessarily provided by a licensed dosimetry service)
- an annual CED greater than 1 mSv and a total annual effective dose greater than 5 mSv (NEWs participating in a routine bioassay program and for whom measurements are provided by a licensed dosimetry service) (RPR, section 8)
In some circumstances, the probability of exceeding 1 mSv per year may be assessed on the basis of the activity handled by the worker, the type of radionuclides involved, the physical and chemical form of the radionuclides, the type of containment used, and the nature of the operations performed. When one type of radionuclide is handled daily (i.e., approximately 250 days per year), workers handling the activities in table 6 should participate in a routine bioassay program. Note that, in order for a decision to be made on participation, bioassay monitoring results from over at least a 2-year period may supersede the data in table 6.
Workers who do not have a reasonable probability of exceeding a CED of 1 mSv per year should also be considered for routine monitoring. However, under paragraph 5(2)(b) of the RPR, the licensee may ascertain doses to these workers by estimation “if the time and resources required for direct measurement as a result of monitoring outweigh the usefulness of ascertaining the amount of exposure and doses using that method”.
The basis for the values in table 6 is presented in appendix B, “Assessing the Activity Handled for Selecting Participants in a Routine Intake Monitoring Program,” and may be used to derive site-specific values. Appendix B defines parameters needed to define the potential intake fraction (PIF). Given a particular scenario of intake, the value ALI/PIF represents the activity handled per day of operation that could result in an annual intake equal to the ALI, consequently resulting in a CED of 20 mSv per year. The criterion set for bioassay participation is 1 mSv/year. Therefore, the data shown in table 6 represent the quantity ALI / (20 × PIF).
| Confinement | Volatility | ||
|---|---|---|---|
| Gases and volatile liquids | Powders | Non-volatile liquids and solids | |
| None | ≥ 2 × ALI | ≥ 20 × ALI | ≥ 200 × ALI |
| Fume hood | ≥ 200 × ALI | ≥ 2,000 × ALI | ≥ 20,000 × ALI |
| Glovebox | ≥ 20,000 × ALI | ≥ 200,000 × ALI | ≥ 2,000,000 × ALI |
| Sealed vials and syringes | ≥ 50 × ALI | Not applicable | ≥ 10,000 × ALI |
When radionuclides are handled less frequently than daily, the values in table 6 may be modified following the method in appendix B.
Bioassay is also recommended for workers who are required to wear respiratory protection equipment specifically to limit the intake of radionuclides.
The category “Sealed vials and syringes” in table 6 applies to sources that meet the following conditions:
- They are handled exclusively in sealed vials and syringes.
- They have a radiological half-life of less than 7 days.
- The handling of radioactivity is more or less uniform throughout the year.
- The radioactive material is not aerosolized, or boiled in an open or vented container.
- The radioactive material is in the form of a dilute liquid solution.
- The radioactive material is contained in a multi-dose vial that is never opened, and amounts are withdrawn only into hypodermic syringes for immediate injection into another multi-dose vial or another form of closed containment, or into patients.
- Contamination control measures are effective, and routine surface monitoring is being carried out where the sealed vials and syringes are handled.
The “Sealed vials and syringes” category is intended to encompass those compounds for which routine bioassay monitoring periods may be impractical due to their short half-life, with additional consideration given to the added containment afforded by the vial as described in item 6 above. Compounds may be classified as “Sealed vials and syringes” provided that the potential for intake is controlled by effective contamination control and the radiation protection measures are effective.
The data in table 6 are provided as generalizations and may not cover all scenarios. In addition, where there are mechanical or other physical barriers in place to protect the worker (such as gloveboxes and fume hoods), the barriers should be appropriate for the nuclear substance being handled, and they should be used as intended and maintained in a proper manner.
When more than one type of radionuclide is handled in one or more chemical forms, or when more than one process can lead to intakes (e.g., involving various containment types or occupancy factors), the following steps should be followed to determine if a worker should participate in a bioassay program:
- Calculate the ratio, rj, of the quantity of one radionuclide, j, handled in daily operation, to the maximum quantity of that radionuclide that can be handled in daily operation above which bioassay is recommended, from table 6.
- Calculate this ratio for all N radionuclides handled.
- Add all of the ratios calculated in steps 1 and 2 above:
(8)
Bioassay should be performed for any radionuclide for which rj ≥ 1. If BT ≥ 1, bioassay should be performed for any radionuclide, chemical form or process for which rj ≥ 0.3. In situations where BT < 1 but any of the rj values are greater than 0.3, the licensee may choose to monitor the worker for these radionuclides. When assessing the need to carry out routine intake monitoring, radioactive impurities that may be present in a product, such as a radiopharmaceutical, should be included in the assessment.
A baseline assessment should be carried out before work requiring routine bioassay monitoring. This assessment determines the worker’s exposure to radionuclides resulting from previous work experience, medical procedures or natural radioactivity in the body.
Baseline bioassay assessment is appropriate for any of the following circumstances:
- The worker has had prior exposure to the pertinent radionuclides and the effective retention in the body might exceed the derived activity (DA) (see section 7.2.5)
- The exposure history is missing or inconclusive.
- The worker will be working with radionuclides that may be detectable in bioassay and that are attributable to non-occupational sources (e.g., radionuclides administered for medical purposes).
7.2.2 Special bioassay monitoring
Special bioassay monitoring is performed in response to a particular circumstance, such as a known or suspected intake of radionuclides due to an abnormal incident in the workplace. Special bioassays are also termed “non-routine” or “ad hoc.” Special bioassay monitoring may be triggered by either a routine monitoring result or an abnormal incident suggesting that an action level (as defined in the RPR) or the dose limit may have been exceeded. Special bioassays may also be triggered by a licensee-defined criterion, such as a worker’s CED exceeding 1 mSv. In such cases, the dose should be ascertained on the basis of case-specific data. Guidance on special bioassay monitoring can be found in appendix C.
7.2.3 Confirmatory monitoring
A confirmatory monitoring program is intended to verify whether:
- assumptions about radiological exposure conditions in the workplace are accurate
- protection measures are effective
- routine bioassay is required
It may involve workplace monitoring or limited individual monitoring of workers who do not meet the criteria for participation in a routine bioassay monitoring program. When workers handle or may be exposed to unsealed radionuclides but do not meet the criteria for participation in a routine bioassay program, intake monitoring may be assessed as part of a confirmatory monitoring program. The monitoring frequency may be the same as for routine monitoring or may vary if potential exposure to the unsealed radionuclides is infrequent (taking into account the biological half-life of the radionuclides).
In a confirmatory monitoring program, workers submit to in vivo or in vitro bioassay, which may involve sampling a fraction of a group of workers. Alternatively, confirmatory monitoring may be carried out using personal air samples collected in the breathing zone. When the results of confirmatory monitoring show that an annual CED of 1 mSv could go undetected without routine monitoring, further measurements should be taken to confirm the intake, and an investigation should be carried out to determine the cause of the unexpected result. If the intake is confirmed, assumptions about radiological exposure conditions in the workplace and the effectiveness of protection measures in place should be reviewed, and the need for involved workers to participate in a routine bioassay program should be re-evaluated. All confirmatory monitoring results should be recorded.
Confirmatory monitoring should be used to review the basis for a routine monitoring program if major changes have been made to the facility or to the operations at the facility. Furthermore, confirmatory monitoring, consisting of using personal air samplers or individual bioassay measurements, should be used to verify that workplace air monitoring results can be considered to be representative.
7.2.4 Task-related monitoring
The purpose of task-related monitoring is to provide information about a particular operation or task and may provide a basis for decisions on the conduct of the operation or task. It is typically used for short-term tasks. Task-related monitoring should be conducted as routine monitoring, unless the circumstances of the operation dictate otherwise, such as if the radionuclides involved may be different or if the probability or potential magnitude of internal exposure may be significantly greater.
7.2.5 Monitoring interval
When selecting a routine monitoring frequency, the main factors to be taken into account are:
- the workplace characteristics
- the uncertainty regarding the time of intake
- instrument sensitivity
- the need for timely information concerning the occurrence of intakes
- the effective half-life of the radionuclides for which monitoring is being carried out
The routine monitoring frequency should be determined on an a priori basis and should consider workers’ likely exposures. For each radionuclide in the workplace, the physical and chemical form should be known for both routine and non-routine monitoring. These forms determine the retention in and clearance from the respiratory tract following inhalation of each radionuclide, as well as their respective excretion routes and rates. The latter will also guide the selection of appropriate bioassay methods.
Guidance on the selection of lung absorption types for various compounds can be found in ICRP Publication 119, Compendium of Dose Coefficients Based on ICRP Publication 60 [11]. Details on the ICRP human respiratory tract model can be found in ICRP Publication 66, Human Respiratory Tract Model for Radiological Protection [15] and its update [13].
Another factor in selecting a routine monitoring frequency is the uncertainty in the intake estimate due to the unknown time of intake. Unless evidence exists supporting a chronic intake pattern, routine measurement results should be assessed in such a way that the intake is assumed to have taken place at the midpoint in the monitoring period.
Instrument sensitivity has a significant impact on the monitoring frequency. The monitoring frequency should be selected so as to ensure that significant doses are not missed. A dose could be missed if, following an intake, the body content or excretion rate of radionuclides taken into the body was reduced to a level less than the instrument’s minimum detectable activity (MDA) during the time between the intake and measurement. The effective half-life is a measure of the rate at which the body content and excretion rate of radionuclides decrease over time after being taken into the body. When practicable, the monitoring period should be such that annual intakes corresponding to a CED of 1 mSv do not go undetected. If this cannot be achieved, workplace monitoring and personal air sampling should be used to supplement intake monitoring. By applying the appropriate metabolic model and assuming a pattern of intake, a suitable monitoring period can be determined.
In order to relate bioassay results to the extrapolated annual dose, the DA has been defined as follows:
(9)
Where:
| T = | the monitoring period, in days |
|---|---|
| m(T/2) = | the contaminated skin surface area in cm2 if the contaminated area is less than the probe surface area and the measurement was taken such that the area of contaminated skin was directly under the probe (if the area is unknown or the skin is unevenly contaminated, 1 cm2 may be conservatively assumed), or the probe’s active surface area in cm2 if skin is evenly contaminated over a larger area than the probe |
| ALI = | The annual limit on intake |
Values of m(T/2) should be obtained based on current Footnote 6 ICRP biokinetic models.
Since the uncertainty resulting from the unknown time of intake relative to the time of monitoring should be less than a factor of 3, the monitoring interval should also satisfy the following condition:
(10)
When the above condition is met, the recommended maximum monitoring period is taken as the time at which the DA is equal to the MDA. If exposures to more than one radionuclide may occur, the monitoring period should be determined so that an annual CED of 1 mSv from all radionuclides can reliably be detected and assessed. The MDA is defined as follows: when the sample or subject count time is different than the background count time. For further information, consult the Health Physics article titled “Minimum Detectable Activity When Background is Counted Longer than the Sample” [16]. Equation 11 applies when the distribution of the net signal is approximately normal. Consequently, equation 11 does not apply to situations in which the number of counts is low. In cases of low-level counters, licensees may refer to reports such as the U.S. Environmental Protection Agency’s Multi-Agency Radiological Laboratory Analytical Protocols Manual (MARLAP), chapter 20 [17].
(11)
In the above equation:
K = a correction factor
Rb = the background count rate
tg = the gross count time (the sample or individual count time)
tb = the background count time
ε = the counting efficiency
For in vitro bioassay:
(12)
Where:
V = the sample size in units of mass or volume, depending on the sample type
Y = the fractional chemical yield, when applicable (no units)
(note: if not applicable, Y=1)
λ = the radioactive decay constant of the radionuclide, in 1/seconds
Δt = the time between sample collection and counting, in seconds
For in vivo bioassay, K is the correction for self-absorption when appropriate
In some cases, the best available monitoring methods may still be unable to reliably detect intakes corresponding to 1 mSv per year. In these circumstances it is useful to determine the maximum dose that could be missed if an intake occurred at the start of each monitoring period. Such an approach provides a useful perspective for some internal hazards that are difficult to detect, but can become overly conservative, particularly when there are several monitoring periods per year.
Using this method for monitoring period determination, a recommended monitoring period of 1 year could be possible for some radionuclides. However, most individuals’ retention and excretion rates tend to vary from the model on which the DA values are based. In addition, timely information about the occurrence of intakes is needed. There should be a balance between using bioassay as an intake indicator and using bioassay for dose assessment purposes. To account for this, a monitoring period shorter than 1 year may be selected depending on other types of monitoring in place (such as workplace air monitoring) and the practicability of carrying out the bioassay measurements. The International Organization for Standardization publication ISO 20553:2006, Radiation Protection – Monitoring of Workers Occupationally Exposed to a Risk of Internal Contamination with Radioactive Material [18], provides suggestions regarding monitoring frequency for various radionuclides and their typical chemical forms.
7.3 Air monitoring to ascertain worker dose
Airborne radioactive material refers to any suspension in air of radioactive material. The characteristics or concentrations may be such that there is no practical means to determine dose through bioassay. Airborne radioactive materials exist in various physical and chemical forms, including dust, gas, fumes and vapours. This section applies to measurements of radioactive material in air that are used for dosimetry purposes. Air monitoring to ascertain worker dose from radon progeny is not considered in this section. Appendix G presents guidance on that topic.
Workplace monitoring methods that may be used to monitor individual intakes of radionuclides include personal air sampling and static air sampling. A personal air sampler (PAS) is a portable device that is worn by an individual. It includes a sampling head containing an appropriate collection medium (e.g., filter), a calibrated air pump, an air flow rate control and a battery. The sampling head should be worn on the upper trunk and in the individual’s breathing zone, which is defined as being within 30 cm of the individual’s head [19]. Air is drawn through the filter by a calibrated pump, also worn by the worker. The activity on the filter should be measured at the end of the wearing period. Static (or fixed-location) air samplers are used to monitor the concentration of radionuclides in the workplace air. A static air sampler (SAS) may consist of a grab sampling device or a continuous monitor. An SAS consists of an appropriate collection medium, an air pump and air flow adjustment. The collection medium may be analyzed in a laboratory. However, some SASs provide real-time monitoring and may be equipped with an alarm set to sound at a predetermined activity or collection rate.
SAS results should be used with caution as a measure of an individual’s intake. Studies have shown that there is a poor correlation between PAS and SAS results, with SAS results generally being an order of magnitude less than PAS results [13]. Studies have also shown a poor correlation between SAS and bioassay results [13]. For further information, consult ICRP Publication 130, Occupational Intakes of Radionuclides: Part I [13]. PAS and SAS measurements may be used as part of a comprehensive workplace monitoring program, as they may provide early identification of possible intakes. Therefore, a personal air sampling program should be designed to detect potential abnormal intakes and to trigger special bioassay measurements. It may also be used to identify potential problem areas with increased airborne radioactivity through review and trending of the applicable static air sampling data.
The concentrations of airborne radioactive material in air are measured in activity or mass per unit volume of that atmosphere (e.g., Bq/m3). The intake (e.g., Bq) from this concentration is calculated by multiplying the concentration by a defined breathing rate (e.g., 1.2 m3/h) and the occupancy time (h). Alternatively, exposure can be determined in Bq h/m3, and the intake will be this value multiplied by the breathing rate. The concentration of airborne radioactive material may also be expressed in units of derived air concentration (DAC). Similarly, exposure may be expressed in terms of DAC-hours.
The flow rate of both personal and static air sampling pumps, where used, should not deviate by more than 5% from the value used to calculate concentration. The airflow rate should be verified each day of air sampler use. If the airflow rate changes by more than ±10% during the collection of a sample, the flow rate used for dosimetry purposes should be the average of the initial and final airflow rates.
Air samplers should have a means of ascertaining the volume of air sampled. Airflow meters must be calibrated, as required by section 25 of the RPR, at least annually, after repairs or modifications have been done to the meter, or if the meter may have been damaged. In addition, at the time of airflow calibration, a verification of air samplers and sampling lines should be carried out to ensure that there is no in-leakage of air upstream of the airflow measurement point. The calibration methods should be based on a current method recommended by the American Conference of Governmental Industrial Hygienists or the U.S. Occupational Safety and Health Administration. The method, the instrument’s unique identifier and the date of calibration should be documented.
The licensee should demonstrate that the air sampled is representative of breathing zone air whenever PASs are not worn within 30 cm of a worker’s head, and (i) the workers’ doses will be ascertained on the basis of air monitoring, and/or (ii) annual exposures are likely to exceed 100 DAC-hours (or the annual CED resulting for inhaled radionuclides is likely to exceed 1 mSv).
This may be accomplished by confirmatory monitoring using bioassay. In order for the air sampling to be considered representative of breathing zone air, the ratio of intakes calculated from air monitoring to the intakes calculated from confirmatory bioassays, averaged over all workers participating in the confirmatory monitoring, should be more than 0.7. The same ratio for each individual worker should be more than 0.5. For further information, consult the U.S. Nuclear Regulatory Commission report NUREG-1400, Air Sampling in the Workplace [19].
Air sampler particle collection efficiency should be insensitive to size to the greatest extent possible. This excludes the use of cyclones to collect and measure airborne radioactive material.
8. Interpreting Monitoring Results
8.1 Administrative levels
Administrative levels are pre-established values that licensees put in place to which measurement quantities from an individual or workplace monitoring program are compared. When such administrative levels are exceeded, specified actions should be taken.
Administrative levels signal potential intakes by workers and allow for a graded response to intakes. They are not intended to be a regulatory limit per se and may be expressed as fractions of the appropriate ALI or CED. When setting administrative levels, the contribution from other radionuclides as well as external exposures should be taken into account. For example, licensees may establish an administrative level that, when exceeded, triggers a confirmation that the intake was in fact real and not due to extraneous factors, such as a contaminated sample.
A set of administrative levels, each associated with a specified potential dose or fraction of an ALI, should be established to allow for a graded response. This set of administration levels should include an investigation level, which triggers the licensee to investigate the cause of a confirmed intake. A bioassay result exceeding an investigation level would indicate a departure from normal conditions and the need to take further action. For routine bioassay programs, investigation levels may be derived assuming the intake occurred at the midpoint in the monitoring period. Furthermore, if applicable, an investigation level should be established to ensure intakes of soluble uranium compounds approaching the threshold for chemical toxicity are investigated.
For some radionuclides and types of bioassay, non-occupational sources may cause typical results to exceed the detection limit and potentially an administrative level. If bioassay results normally or often exceed an administrative level due to non-occupational sources, such as from naturally occurring radionuclides, the administrative level may be increased if expected bioassay results attributable to non-occupational sources are known (a study using a control group with similar non-occupational exposure but no potential for occupational exposure may be used for this purpose). If non-occupational levels exceed the investigation level, then alternative methods of intake monitoring should be used if possible.
The investigation level should be based on a pre-determined dose not exceeding 5 mSv per year. When there is a probability of intake that is more or less uniform throughout the year, the investigation level should be derived from a pro-rated annual dose, as described by equation 13, and should reflect levels of exposure representing a departure from normal conditions.
When doses are generally low and the processes are well known, investigation levels should be selected on the basis of experience, so that exceeding an investigation level would be a departure from normal conditions and would warrant an investigation. In this case, the investigation level would be based on an annual dose of less than 5 mSv, and should be revised on the basis of operational experience.
Because bioassay monitoring programs do not directly measure intakes or CED, derived administrative levels expressed in terms of the quantity that is measured are generally a more useful quantity. The derived level corresponding to the investigation level is the derived investigational level (DIL), which may be defined as follows for a routine monitoring program:
(13)
Where:
| IL = | the intake leading to the annual CED above which an investigation should be carried out, that is, an investigational level |
|---|---|
| T = | the routine monitoring period, in days |
| m(ᵀ⁄2) = | the fraction of the intake that is retained in a tissue, organ or the whole body, or excreted from the body, at the end of the monitoring period, when an acute intake has occurred at the midpoint in the monitoring period |
If the DIL is less than the detection limit, an investigation should be carried out whenever the detection limit is exceeded.
To account for the reduced dose limit for pregnant workers, a DIL for pregnant workers should be established, as described above, on the basis of a fraction of the 4 mSv dose limit for NEWs. The pregnant worker dose limit is 4 mSv for the balance of the pregnancy (that is, from the time the worker informs the licensee). Given conservative assumptions (for example, that the pregnancy is declared immediately), ensuring that the pregnant worker’s dose is < 0.4 mSv per month helps to ensure the 4 mSv limit is not exceeded. Consequently, a DIL for pregnant workers, DILPW, may be set as:
(14)
In cases of intakes of more than one radionuclide, the administrative level should consider the dose from the mixture of radionuclides. This approach may be used when monitoring is done using one radionuclide as an indicator for a mixture of radionuclides.
When an investigation level, or the corresponding DIL, has been exceeded, the following actions should be taken, where relevant.
- Remove the involved workers from work that could result in additional intakes.
- Determine, to the extent possible, the characteristics of the intake, including the time of intake and the characteristics of the material taken in.
- Initiate special bioassay, as described in appendix C.
- Review the circumstances relevant to the intake to identify and correct the causes of the intake and prevent recurrence. The investigation should also consider the corrective actions to be taken.
8.2 Accuracy of bioassay results
Measurement uncertainties arise from counting statistics and other sources that depend on the monitoring method. In the case of in vivo measurements, measurement uncertainties may arise from such sources as variations in the detector positioning, in the background count rate, in subject body size and in the distribution of activity within the body. In the case of in vitro measurements, such uncertainties can arise from the measurement of the sample volume or mass, pipetting errors, the use of tracers to determine chemical yield, and other causes.
Measurement uncertainties resulting from counting statistics, which can be described by the Poisson distribution, are referred to as Type A uncertainties. All other uncertainties are referred to as Type B uncertainties. The overall uncertainty over an individual monitoring result may be described in terms of a log-normal distribution. The geometric standard deviation of this distribution is called the scattering factor (SF). For further information, consult European Radiation Dosimetry Group (EURADOS) Report 2013-01, IDEAS Guidelines (Version 2) for the Estimation of Committed Doses from Incorporation Monitoring Data [20].
For Type A uncertainties, the SF may be calculated as follows:
(15)
In the above equation, σA is the Type A uncertainty of measurement result M.
The SF for Type B uncertainties may be calculated as follows:
(16)
In the above equation, Crn is the normalization factor, which is the reciprocal of the efficiency, and sCrn is the uncertainty on Crn. Typical values of SF for Type A and B uncertainties are shown in tables 7 and 8, taken from EURADOS Report 2013-01 [20]. The total uncertainty may be calculated using the following equation:
(17)
| Scattering factor (SF) | |||
|---|---|---|---|
| Photon energies less than 20 keV | Photon energies from 20 keV to 100 keV | Photon energies greater than 100 keV | |
| Type A uncertainties | 1.5 | 1.3 | 1.07 |
| Type B uncertainties | 2.06 | 1.25 | 1.15 |
| Total SF | 2.3 | 1.4 | 1.2 |
| Quantity | Scattering factor (SFB) |
|---|---|
| True 24-hour urine sample | 1.1 |
| Activity concentration of tritiated water in urine | 1.1 |
| Simulated 24-hour urine, creatinine, volume or specific gravity normalized | 1.6 |
| Spot urine sample (a single void used to estimate the 24-hour excretion rate) | 2 |
| Fecal 24-hour sample | 3 |
| Fecal 72-hour sample | 2 |
The complete bioassay measurement system should be such that any error in the final measurement would have a minor influence on the overall accuracy of the estimated radiation dose received by the worker. The following considerations should be included in the evaluation of detection instrument accuracy and measurement methodology:
- The net statistical counting error: This includes the statistical error in the bioassay count and the statistical error in the measurement of the background count. The background count time should be appropriate for the standard, sample or subject.
- The error caused by variations in counting geometry: This should include allowances for physical variations in the subjects or samples being counted, particularly as related to the specific counting equipment being used.
- The error introduced by the attenuation of the emitted radiation by overlying tissue during in vivo counting: The effect of overlying tissue should be considered where the gamma emission of the nuclide in question is less than 200 keV, or where bremsstrahlung from beta emissions are being counted; this requires the estimation of the average depth and density of the overlying tissue (e.g., the chest wall thickness), which may vary significantly from one individual to another.
- The instrument calibration with respect to the nuclear substance being measured in a geometry that is relevant to the actual measurement: The response of the bioassay instrument should be calibrated with respect to the nuclear substance of interest, and a regular quality control program should be in place to ensure that this calibration is constantly maintained. Frequent internal checks using a long‑lived radioactive source should be performed on a regular basis to confirm that the detector response is constant over time and that the instrument is functioning properly.
9. Ascertaining the Committed Effective Dose
When the time between the intake and a single bioassay measurement is known, the intake should be calculated as follows:
(18)
In this case, I represents the intake (for example, in Bq or mg); M is the measured quantity; and m(t) is the predicated value of retention or excretion functions at a time, t, after the intake. The value of m(t) is based on appropriate biokinetic models and is available for default solubility characteristics for the material from the ICRP. Values of m(t) may also be derived for material‑specific solubility or particle sizes. The measured quantity and m(t) should be expressed in consistent units. For example, for urinalysis, M should be the activity of the radionuclide of interest excreted per day at the end of the sample collection period, while m(t) is the urinary excretion rate of the same radionuclide at the end of the sample collection period. The latter scenario typically applies in special or task-related monitoring.
In routine monitoring, the time between an intake and the bioassay monitoring may not be known. In such cases, the CED may be ascertained by assuming that the intake occurred at the midpoint in the monitoring period of T days. The intake should be calculated as follows, based on the measured quantity at the end of the monitoring period:
(19)
In both cases above, the CED may be ascertained by multiplying the intake by the appropriate CED per unit intake. In some instances, as with tritiated water, measurements of activity may be used to ascertain the effective dose directly. In such cases, the above method may be replaced by a method presented for specific radionuclides in the appendices, or as approved by the CNSC.
If more than about 10% of the actual measured quantity can be attributed to intakes in a previous monitoring interval, a correction may be made. The correction to the current monitoring interval’s measured quantity may be done by:
- determining the intake in the previous monitoring interval
- using the appropriate m(t) to predict the contribution of the previous intake to the current measured quantity
- subtracting the contribution as calculated above from the current measured quantity
In some circumstances, including special bioassay monitoring, individual monitoring results taken at various times and using multiple monitoring methods (e.g., in vitro and in vivo bioassay) may be available. In these cases, the best estimate of the intake should be calculated by determining:
- the value of mj(ti) for each monitoring result and for each monitoring method
- the best estimate of the intake, such that I × mj(ti) best fits the measurement results Mi, j
When multiple monitoring methods are used, the intake should be ascertained by fitting predicted values (I × mj(ti)) to the results from all monitoring methods simultaneously. For example, urine and fecal bioassay data sets may be obtained as part of a special bioassay monitoring campaign. The intake in this case should be ascertained by fitting the predicted values (I × mj(ti)) to both data sets simultaneously. Statistical methods are available for data fitting; the 2 most commonly used for bioassay are the maximum likelihood method and Bayesian approach. These, as well as others, are described in IAEA Safety Reports Series No. 37, Methods for Assessing Occupational Radiation Doses due to Intakes of Radionuclides [21], and EURADOS Report 2013-01: IDEAS Guidelines (Version 2) for the Estimation of Committed Doses from Incorporation Monitoring Data [20].
When ascertaining an intake from data fitting, the starting assumption is that the data are consistent with the biokinetic model; that is, the measurement results Mi, j are consistent with the predictions I × mj(ti). The criteria for rejecting the fit may be based on the chi-squared test statistic, and each measurement Mi, j may be assumed to be taken from a lognormal distribution. The fit to the data should be judged to be inadequate if the p-value is less than 0.05. The p-value is the fraction of the expected (theoretical) c2 distribution that is greater than the calculated co2 value. More information on the criteria for rejecting a data fit in the context of bioassay may be found in EURADOS Report 2013-01 [20].
When the fit is rejected and the estimated intake leads to a CED > 1 mSv, the material-specific absorption parameters from the ICRP human respiratory tract model may be adjusted. For further information, consult ICRP Publication 66, Human Respiratory Tract Model for Radiological Protection [15]. Specifically, the time of intake and routes of intake, if not known, may be varied to improve the fit. In addition, the values of fr and ss may be varied, but not the value of sr Footnote 7 (which should be kept at the value recommended by the ICRP) until the fit is not rejected [20].
The method for ascertaining the CED may differ or include some additional factors during consideration of specific radionuclides. Recommendations specific to tritium, radioiodines and uranium are discussed in appendices D to F, respectively.
10. Calibration
Instruments used for in vivo or in vitro bioassay measurements must be selected, tested and calibrated periodically as required by section 25 of the RPR. Calibration must be performed for the nuclear substance measured in the bioassay program. Periodic calibration and maintenance requirements must be determined and documented based on the necessary accuracy, purpose, degree of usage, stability characteristics and other factors affecting measurement control. Maintenance and calibration procedures should be documented.
A record of calibration must be maintained, and calibrated equipment should be clearly and indelibly identified (e.g., through the use of labels). When calibration is performed before use or with a high frequency (e.g., daily), logging of calibrations may be sufficient.
Inaccurate, uncalibrated or malfunctioning equipment should be identified and removed from use. Measurement equipment that has been repaired or modified should be calibrated and have its performance checked before being put into use.
Calibrations should be traceable to national reference standards. Equipment used as calibration transfer standards should have calibration traceable to national standards. Where calibrated reference standards are used as transfer standards to set the level of reference by which data are directly measured, methods should be established to preserve the integrity of the process and the results.
When equipment is found to be inaccurate, reviews should be conducted to determine the validity of data or results, and corrective action should be taken.
11. Limiting Intakes of Nuclear Substances by Workers Who Are Breastfeeding
The RPR require licensees to make accommodations to limit intakes of nuclear substances by a NEW who is breastfeeding. Section 11 of REGDOC-2.7.1 [1] provides guidance regarding NEWs who are breastfeeding. In particular, when a licensee is informed in writing that a NEW is breastfeeding, the licensee must make any accommodation that will not cause undue financial hardship or business inconvenience. The licensee may need to implement administrative controls for a breastfeeding NEW to ensure that intakes of nuclear substances by the NEW, which can subsequently be transferred to the breastfed infant, are minimized. Administrative controls may include ensuring that the working conditions are such that there is no significant risk of intake of nuclear substances. Consequently, breastfeeding NEWs who do not participate in a routine monitoring bioassay program due to the low risk of intakes should undergo confirmatory monitoring to confirm that there have been no intakes.
In the event of an intake, the magnitude of the intake should be estimated to ensure that the dose (CED) to the breastfed infant does not exceed 1 mSv. As a rule of thumb for most nuclear substances, if inhalation intakes of nuclear substances by NEWs who are breastfeeding are controlled to keep the annual CED below 1 mSv to the NEW, then the breastfed infant will not receive a CED above 1 mSv per calendar year from these intakes. There are exceptions in which intakes of certain nuclear substances (such as S-35, radioiodines and tritiated water) by the NEW may result in a CED of more than 1 mSv to the breastfed infant relative to the dose received by the NEW.
Licensees should compare dose coefficients for NEWs with those for breastfed infants (ICRP Publication 95: Doses to Infants from Ingestion of Radionuclides in Mothers’ Milk [22]) for nuclear substances relevant to their facilities to verify that doses to breastfed infants do not pose a risk to the infant and are maintained below dose limits. ICRP Publication 100, Errata to: Doses to Infants from Ingestion of Radionuclides in Mothers’ Milk (ICRP Publication 95, Ann. ICRP 34(3/4)) [23], should also be consulted for corrections to the Tc-99m, thorium and uranium tables.
The ratios of the CED received by a breastfed infant to the corresponding CED received by the breastfeeding NEW after an acute inhalation intake are shown in table 9 for selected nuclear substances. In order to estimate the dose to a breastfed infant in circumstances where the worker continues to breastfeed following an intake, the CED to a breastfeeding NEW may be multiplied by the appropriate ratio in table 9 to obtain the CED to the breastfed infant. These ratios were derived assuming occupational intakes by inhalation for the most conservative inhalation type or compound type (e.g., vapour in the case of I-131). In cases where an intake by ingestion is suspected, ratios for ingestion dose coefficients should be calculated from the appropriate occupational dose coefficients for adults and for the nursing infant. This method may be used to verify that the dose to a breastfed infant, from all nuclear substances taken in by the breastfeeding NEW, is maintained at less than 1 mSv per calendar year. The factors shown in table 9 assume breastfeeding continues for 6 months. If there has been an intake and breastfeeding is expected to continue for more than 6 months, the licensee should consult with the CNSC to determine appropriate dose coefficients.
| Nuclear substance | Ratio |
|---|---|
| 3H (water) | 1.1 |
| 14C | 0.33 |
| 32P | 0.81 |
| 33P | 0.63 |
| 35S | 1.2 |
| 45Ca | 0.38 |
| 47Ca | 0.35 |
| 55Fe | 0.015 |
| 59Fe | 0.0075 |
| 60Co | 0.20 |
| 95Zr | 0.0047 |
| 95Nb | 0.00015 |
| 99mTc | 0.49 |
| 125I | 1.1 |
| 131I | 2.6 |
| 134Cs | 0.10 |
| 137Cs | 0.13 |
| 210Pb | 0.27 |
| 210Po Footnote 8 | 0.020 |
| 226Ra | 0.0073 |
| 238U | 0.0079 |
| 241Am | 0.00022 |
| 238Pu | 0.00024 |
| 239Pu | 0.00023 |
| 244Cm | 0.00027 |
12. Ascertaining the Dose Resulting From an Intake of Nuclear Substances via a Wound
Intakes of radionuclides via a wound are assessed in the context of special bioassay monitoring. The purpose of these bioassay measurements is to ensure compliance with dose limits and to inform decisions regarding patient treatment (e.g., excision of the wound, decorporation). In addition to bioassay measurements, special monitoring should include measurements of local activity at the wound site.
The selection of monitoring methods depends on the type of wound (e.g., puncture, laceration, thermal burn), the category of wound contaminant (e.g., radionuclides in solution, particles, fragments) and the biokinetics of the radionuclide. While soluble compounds are rapidly transferred to blood, insoluble compounds may be retained at the wound site, and a fraction may be translocated to regional lymph nodes, remaining at both these locations for an extended period of time.
The biokinetics of specific compounds taken in through a wound depend on the type of wound and its physiological evolution (e.g., healing). In general, the proportion of a soluble compound absorbed to blood from a wound site decreases in the following order:
- intravenous injection (greatest proportion of compound absorbed to blood)
- puncture wounds
- lacerations and abrasions
- burned skin (thermal or chemical)
- intact skin (smallest proportion of compound absorbed to blood)
Categories of wound contaminants are defined in National Council on Radiation Protection and Measurements (NCRP) Report No. 156, Development of a Biokinetic Model for Radionuclide‑Contaminated Wounds and Procedures for Their Assessment, Dosimetry and Treatment [24]. The categories are:
-
radionuclides initially in solution
- weak retention at the wound site (up to 10% of initial activity remains at the wound site 24 hours after wound intake)
- moderate retention at the wound site (10% to 30% of initial activity remains at the wound site 24 hours after wound intake)
- strong retention at the wound site (30% to 80% of initial activity remains at the wound site 24 hours after wound intake)
- avid retention at the wound site (more than 80% of initial activity remains at the wound site 24 hours after wound intake)
-
radionuclides initially insoluble in water
- colloids
- particles
- fragments
Particles and fragments are solids. They, as well as colloids, can be deposited in lymph nodes after clearing from the wound site.
The following steps should be followed when monitoring a contaminated wound:
-
The wound contamination should be characterized by documenting:
- the date, time, and method and circumstances of the wound contamination incident
- the type, characteristics and location of the wound
- the characteristics of the radiological contaminant at the wound site, including the radionuclides, their chemical form and total activity or concentration
- The activity deposited at the wound site should be measured as soon as practicable after the wound incident and periodically afterwards, as this will help guide the medical management of the case. Follow-up measurements are recommended in order to gauge the effectiveness of decontamination and medical interventions. Guidance on the selection of instruments for wound monitoring can be found in NCRP Report No. 156 [24].
- An in vitro or in vivo bioassay measurement should be carried out, as appropriate, for the radionuclides and their associated chemical forms as determined in step 1 as soon as practicable after the wound incident and periodically afterwards according to the frequency set out in appendix C.
- The equivalent dose to skin at the wound site should be ascertained based on information obtained through steps 2 and 3 where feasible.
- The CED from intakes of radionuclides through the wound should be ascertained.
The equivalent dose to tissue at the wound site should be ascertained to determine whether tissue reactions are likely, and to verify compliance with the equivalent dose limit for the skin. Once the activity deposited at the wound site has been ascertained, an initial conservative estimate may be carried out. This may be done by multiplying the activity concentration at the wound site by the appropriate skin dose conversion factor, listed in table 10.
| Radionuclide | Equivalent dose rate received by the skin (mSv.h-1.kBq-1.cm2) | |
|---|---|---|
| Surface contamination | Deep contamination | |
| 3H | 0 | 1.3×10-3 |
| 14C | 3.2×10-1 | 1.8 |
| 22Na | 1.7 | 3.2 |
| 32P | 1.9 | 4.2 |
| 35S | 3.5×10-1 | 1.7 |
| 36Cl | 1.8 | 3.2 |
| 45Ca | 8.5×10-1 | 2.2 |
| 51Cr | 1.5×10-2 | 2.7×10-2 |
| 54Mn | 6.2×10-2 | 8.1×10-2 |
| 57Co | 1.2×10-1 | 1.9×10-1 |
| 58Co | 3.1×10-1 | 5.6×10-1 |
| 60Co | 7.8×10-1 | 3.2 |
| 59Fe | 9.6×10-1 | 3.3 |
| 63Ni | 6.5×10-7 | 4.5×10-1 |
| 67Ga | 3.4×10-1 | 1.1 |
| 90Sr, 90Y | 3.6 | 7.9 |
| 95Zr, 95Nb | 1.6 | 4.3 |
| 99mTc | 2.5×10-1 | 4.0×10-1 |
| 106Ru, 106Nb | 2.2 | 6.5 |
| 110mAg | 6.7×10-1 | 1.9 |
| 111In | 3.8×10-1 | 6.7×10-1 |
| 123I | 3.7×10-1 | 6.8×10-1 |
| 125I | 2.1×10-2 | 3.5×10-1 |
| 131I | 1.6 | 3.1 |
| 137Cs, 137mBa | 1.6 | 3.4 |
| 144Ce, 144mPr, 144Pr | 3.1 | 8.2 |
| 147Pm | 6.0×10-1 | 2.0 |
| 192Ir | 1.9 | 3.4 |
| 201Tl | 2.8×10-1 | 1.0 |
| 204Tl | 1.6 | 3.0 |
| 235U | 1.8×10-1 | 3.0×103 |
| 238U | 2.3×10-3 | 2.9×103 |
| 238Pu | 3.7×10-3 | 3.4×103 |
| 239Pu | 1.4×10-3 | 3.2×103 |
| 241Pu | 1.3×10-5 | 8.0×10-2 |
| 241Am | 2.0×10-2 | 3.4×103 |
The radionuclides may be assumed to be surface contamination in the case of chemical burns or abrasions. In other cases, unless evidence exists for surface contamination, the radionuclides should be assumed to be retained as deep contamination. For a more accurate dose assessment, skin dosimetry software should be used.
An upper bound to the CED may be calculated by assuming all of the activity at the wound site will be taken up into the blood. Dose coefficients for selected radionuclides for this purpose are shown in table 11 under the “Weak” heading. Once bioassay measurement results become available, they should be used to ascertain the CED. The bioassay measurements may be corrected to account for previous intakes of radionuclides.
For cases in which the activity is cleared rapidly from the wound site (e.g., less than 10% of the activity measured in step 2 immediately following the wound contamination incident remains at the wound site 24 hours later), the intake may be treated as an injection intake. The intake can be ascertained using the equation in section 11:
(20)
The parameter m(t) is the predicted activity in the bioassay measurement per unit intake. These parameters can be obtained from ICRP Publication 78: Individual Monitoring for Internal Exposure of Workers: Replacement of ICRP Publication 54 [25], or ISO 27048:2011: Radiation Protection – Dose Assessment for the Monitoring of Workers for Internal Radiation Exposure [26]. The CED may then be determined by calculating I × einj(50). The latter parameter, the dose coefficient for an injection intake, may be obtained from table 11, under the “Weak” heading, or calculated using internal dosimetry software incorporating ICRP biokinetic models. The criteria defining the categories of wound contaminants, as described above, may be used to determine which heading under table 11 to use. For more guidance, see NCRP Report No. 156 [24]. The data in table 11 was sourced from the Health Physics article, “Dose Coefficients for Intakes of Radionuclides via Contaminated Wounds” [27].
For cases in which the activity is retained at the wound site, as determined by measurements at the wound site in the first few days after the wound contamination incident, the CED should be ascertained using the wound biokinetic model from NCRP Report No. 156 [24] or using another model approved by the CNSC. An initial assessment using an NCRP wound model category chosen a priori may be carried out. When bioassay monitoring data become available, the CED should be ascertained for the wound category that best fits the excretion and/or retention data. If the goodness of fit is not acceptable with 1 wound category, based on the criteria in section 9, the dose should be calculated considering a mixture of 2 default retention categories.
| Radionuclide | Weak | Moderate | Strong | Avid | Colloid | Particle | Fragment |
|---|---|---|---|---|---|---|---|
| 3H (HTO) | 1.84 × 10-11 | 1.84 × 10-11 | 1.78 × 10-11 | 1.61 × 10-11 | 1.56 × 10-11 | 1.01 × 10-11 | 4.07 × 10-13 |
| 3H (OBT) | 4.16 × 10-11 | 4.16 × 10-11 | 4.01 × 10-11 | 3.64 × 10-11 | 3.52 × 10-11 | 2.28 × 10-11 | 9.19 × 10-13 |
| 14C | 5.77 × 10-10 | 5.77 × 10-10 | 5.75 × 10-10 | 5.68 × 10-10 | 5.77 × 10-10 | 5.71 × 10-10 | 3.19 × 10-11 |
| 32P | 2.20 × 10-9 | 2.00 × 10-9 | 1.32 × 10-9 | 4.61 × 10-10 | 1.14 × 10-10 | 6.13 × 10-12 | 6.53 × 10-12 |
| 35S (inorganic) | 1.24 × 10-10 | 1.20 × 10-10 | 9.11 × 10-11 | 3.44 × 10-11 | 1.86 × 10-11 | 1.44 × 10-12 | 2.95 × 10-13 |
| 35S (organic) | 7.76 × 10-10 | 7.51 × 10-10 | 5.70 × 10-10 | 2.15 × 10-10 | 1.16 × 10-10 | 9.01 × 10-12 | 1.85 × 10-12 |
| 59Fe | 8.36 × 10-9 | 7.95 × 10-9 | 5.73 × 10-9 | 1.99 × 10-9 | 8.56 × 10-10 | 5.43 × 10-11 | 1.08 × 10-11 |
| 57Co | 6.36 × 10-10 | 6.28 × 10-10 | 5.16 × 10-9 | 4.01 × 10-10 | 1.84 × 10-10 | 2.45 × 10-11 | 3.00 × 10-12 |
| 58Co | 1.53 × 10-9 | 1.47 × 10-9 | 1.10 × 10-9 | 4.01 × 10-10 | 2.03 × 10-10 | 1.46 × 10-11 | 3.07 × 10-12 |
| 60Co | 1.94 × 10-8 | 1.94 × 10-8 | 1.81 × 10-8 | 1.49 × 10-8 | 1.38 × 10-8 | 6.11 × 10-9 | 2.47 × 10-10 |
| 85Sr | 1.10 × 10-9 | 1.06 × 10-9 | 7.86 × 10-10 | 2.83 × 10-10 | 1.39 × 10-10 | 9.77 × 10-12 | 2.05 × 10-12 |
| 89Sr | 3.13 × 10-9 | 2.98 × 10-9 | 2.17 × 10-9 | 7.61 × 10-10 | 3.43 × 10-10 | 2.24 × 10-11 | 4.59 × 10-12 |
| 90 Sr | 8.80 × 10-8 | 8.81 × 10-8 | 8.66 × 10-8 | 8.26 × 10-8 | 8.22 × 10-8 | 6.57 × 10-8 | 2.87 × 10-9 |
| 99mTc | 1.50 × 10-11 | 1.17 × 10-11 | 3.21 × 10-12 | 3.41 × 10-12 | 1.50 × 10-14 | 1.34 × 10-15 | 6.91 × 10-19 |
| 106Ru | 3.02 × 10-8 | 2.99 × 10-8 | 2.51 × 10-8 | 1.39 × 10-8 | 1.04 × 10-8 | 1.67 × 10-9 | 1.65 × 10-10 |
| 125I | 1.54 × 10-8 | 1.48 × 10-8 | 1.09 × 10-8 | 3.90 × 10-9 | 1.87 × 10-9 | 1.28 × 10-10 | 2.68 × 10-11 |
| 129I | 1.07 × 10-7 | 1.07 × 10-7 | 1.06 × 10-7 | 1.05 × 10-7 | 1.07 × 10-7 | 1.06 × 10-7 | 5.87 × 10-9 |
| 131I | 2.13 × 10-8 | 1.88 × 10-8 | 1.19 × 10-8 | 4.35 × 10-9 | 7.36 × 10-10 | 3.85 × 10-11 | 2.45 × 10-12 |
| 134Cs | 1.94 × 10-8 | 1.94 × 10-8 | 1.71 × 10-8 | 1.16 × 10-8 | 9.70 × 10-9 | 2.45 × 10-9 | 1.48 × 10-10 |
| 137Cs | 1.36 × 10-8 | 1.36 × 10-8 | 1.34 × 10-8 | 1.28 × 10-8 | 1.27 × 10-8 | 1.03 × 10-8 | 4.77 × 10-10 |
| 192Ir | 6.67 × 10-9 | 6.43 × 10-9 | 4.82 × 10-9 | 1.77 × 10-9 | 9.09 × 10-10 | 6.65 × 10-11 | 1.39 × 10-11 |
| 201Tl | 8.34 × 10-11 | 6.91 × 10-11 | 4.11 × 10-11 | 1.70 × 10-12 | 1.29 × 10-12 | 6.83 × 10-14 | 1.50 × 10-15 |
| 210Po | 2.36 × 10-6 | 2.31 × 10-6 | 1.81 × 10-6 | 7.52 × 10-7 | 4.60 × 10-7 | 4.31 × 10-8 | 7.72 × 10-9 |
| 226Ra | 1.36 × 10-6 | 1.36 × 10-6 | 1.44 × 10-6 | 1.62 × 10-6 | 1.77 × 10-6 | 2.64 × 10-6 | 1.65 × 10-7 |
| 228Ra | 3.37 × 10-6 | 3.96 × 10-6 | 1.41 × 10-5 | 3.81 × 10-5 | 4.56 × 10-5 | 4.04 × 10-5 | 1.13 × 10-6 |
| 228Th | 1.18 × 10-4 | 1.17 × 10-4 | 1.03 × 10-4 | 6.86 × 10-5 | 5.68 × 10-5 | 1.37 × 10-5 | 8.64 × 10-7 |
| 230Th | 4.19 × 10-4 | 4.19 × 10-4 | 4.13 × 10-4 | 3.99 × 10-4 | 3.99 × 10-4 | 3.35 × 10-4 | 1.44 × 10-5 |
| 232Th | 4.52 × 10-4 | 4.52 × 10-4 | 4.48 × 10-4 | 4.40 × 10-4 | 4.47 × 10-4 | 4.17 × 10-4 | 1.92 × 10-5 |
| 234U | 2.27 × 10-6 | 2.27 × 10-6 | 2.25 × 10-6 | 2.18 × 10-6 | 2.19 × 10-6 | 1.92 × 10-6 | 8.75 × 10-8 |
| 235U | 2.11 × 10-6 | 2.11 × 10-6 | 2.09 × 10-6 | 2.03 × 10-6 | 2.04 × 10-6 | 1.78 × 10-6 | 8.13 × 10-8 |
| 238U | 2.03 × 10-6 | 2.03 × 10-6 | 2.01 × 10-6 | 1.96 × 10-6 | 1.97 × 10-6 | 1.73 × 10-6 | 7.89 × 10-8 |
| 237Np | 2.05 × 10-4 | 2.05 × 10-4 | 2.03 × 10-4 | 1.98 × 10-4 | 1.99 × 10-4 | 1.76 × 10-4 | 7.91 × 10-6 |
| 238Pu | 4.44 × 10-4 | 4.43 × 10-4 | 4.36 × 10-4 | 4.18 × 10-4 | 4.17 × 10-4 | 3.36 × 10-4 | 1.41 × 10-5 |
| 239Pu | 4.89 × 10-4 | 4.89 × 10-4 | 4.83 × 10-4 | 4.66 × 10-4 | 4.67 × 10-4 | 3.90 × 10-4 | 1.67 × 10-5 |
| 240Pu | 4.89 × 10-4 | 4.89 × 10-4 | 4.83 × 10-4 | 4.66 × 10-4 | 4.67 × 10-4 | 3.90 × 10-4 | 1.67 × 10-5 |
| 241Pu | 9.40 × 10-6 | 9.40 × 10-6 | 9.42 × 10-6 | 9.46 × 10-6 | 9.68 × 10-6 | 9.23 × 10-6 | 4.10 × 10-7 |
| 241Am | 3.97 × 10-4 | 3.96 × 10-4 | 3.91 × 10-4 | 3.79 × 10-4 | 3.80 × 10-4 | 2.23 × 10-4 | 1.41 × 10-5 |
| 242Cm | 1.35 × 10-5 | 1.33 × 10-5 | 1.09 × 10-5 | 5.66 × 10-6 | 4.22 × 10-6 | 1.66 × 10-6 | 1.02 × 10-7 |
| 244Cm | 2.34 × 10-4 | 2.34 × 10-4 | 2.27 × 10-4 | 2.11 × 10-4 | 2.06 × 10-4 | 1.44 × 10-4 | 5.72 × 10-6 |
| 252Cf | 1.52 × 10-4 | 1.51 × 10-4 | 1.36 × 10-4 | 9.79 × 10-5 | 8.43 × 10-5 | 2.49 × 10-5 | 1.30 × 10-6 |
Part C – Making Changes to Dose-Related Information Filed With the National Dose Registry
13. General Process
The CNSC uses dose records to monitor licensee compliance with regulatory occupational dose limits. To that effect, it is important that the doses submitted to the NDR be current and accurate to the extent possible. Dose information filed with the NDR may be changed for various reasons (e.g., following an investigation that concludes there is an incorrect dose record). The following steps describe the general process for a licensee to request, when justified, a change to a dose record filed with the NDR:
- The licensee submits to the CNSC the investigation report and the dose information change request form, which includes details of the change(s) to be made.
- The CNSC evaluates the request and approves or denies it based on the information provided in the investigation report.
- If the CNSC approves the requested change, the dose information change request form is sent to the dosimetry service provider, with a copy of the form sent to the worker, the licensee contact and the NDR. The dosimetry service provider is responsible for notifying the NDR of the change.
- If the CNSC denies the request, the licensee is informed of the refusal.
14. Individual Dose Information Change Request Procedure
-
The licensee conducts an investigation of the event that prompted the request for a dose information change and
summarizes the information in an investigation report, which should contain the following information:
- reasons for requesting the dose information change
- description of the circumstances and time frame involved
- justification for changing the reported dose(s) to the proposed value(s)
- calculations to support the request, if applicable
- copy of the relevant section of the dosimetry service dose report
- other relevant information, as determined by the CNSC
-
The licensee provides the following information in section A of the
dose information change request form:
- dosimetry service name and group or account number that is assigned to the licensee by the dosimetry service
- company name that appears on the dosimetry service dose report
- licensee name that appears on the CNSC licence
- licence number that appears on the CNSC licence
- the worker’s name and social insurance number
- whether the worker is a nuclear energy worker
- serial number of the dosimeter that is shown on the original dose report, if applicable
- wearing period or monitoring period as listed on the original dose report, if applicable
- the requested dose information change
- investigation report as described in step 1
- The worker whose dose information will be affected signs and dates “Section B – Worker Declaration” of the dose information change request form. If the worker cannot be located, the licensee should demonstrate that every effort was made to contact the worker. In some cases, CNSC staff may approve the dose information change request without the worker’s signature. These situations are assessed on a case-by-case basis.
- The licensee submits the completed dose information change request form and any attachments to the attention of the CNSC single point of contact for the licence.
- CNSC staff complete, date and sign “Section A – Licensee Declaration” of the dose information change request form.
- The licensee informs the affected worker of any change to the dose information.
If the licensee submits a request to add the skin dose, as determined in section 5.3.4, to the worker’s dose records in the NDR, the request should be in the form of a dose information change request. The following information should also be included with the dose change request:
- the contamination meter’s make, model and calibration certificate
- a detailed description of how the detector efficiency was determined
- a detailed dose calculation, including measurement times and results
15. Group Dose Information Change Request Procedure
There may be situations in which dose information change requests are required for a large number of individuals and providing dose information change request forms for each individual is not practical. In these situations, the licensee may provide the required information in another format, such as a table, to accommodate the large number of workers to whom the dose information change request applies.
The licensee should demonstrate that every effort was made to inform each worker of the change and that each worker agrees to the proposed change(s) to their dose records.
The licensee is also required to provide an investigation report as described in section 14.
16. Contact Information
The investigation report and the dose information change request form should be submitted to:
Canadian Nuclear Safety Commission
P.O. Box 1046, Station B
280 Slater Street,
Ottawa, Ontario
K1P 5S9
Telephone: 1-888-229-2672
Fax: 613-995-5086
Appendix A: Guidance on Choosing Dosimetry for the Lens of the Eye
Tables A.1 and A.2 provide guidance on choosing the appropriate dosimetry to monitor dose to the lens of the eye. These tables represent simplifications of a complex topic, and are provided as general guidance. It is possible that licensees may have information for their particular circumstances that is more appropriate or advanced. The operational quantities and types of dosimeters listed below may not be the optimal choice in all cases.
Alpha particles and other high linear energy transfer (LET) radiation have not been considered here in view of their limited range in tissue. Furthermore, neutron radiation has not been included in the table; guidance on that topic is provided in section 4.6.
| Mean energy ≥ 40 keV | Mean energy < 40 keV | Angle of incident radiation1 | Is the body uniformly exposed? | Recommended operational quantity | Recommended dosimeter type and placement |
|---|---|---|---|---|---|
| - | Yes | Not applicable | Yes | Hp(0.07) |
|
| - | Yes | Not applicable | No, eyes preferentially exposed | Hp(0.07) |
|
| Yes | - | Radiation is coming from the front or the person is moving about in the field3 | Yes | Hp(0.07) or Hp(10) |
|
| Yes | - | Radiation is coming from the front or the person is moving about in the field3 | No, eyes preferentially exposed | Hp(0.07) or Hp(10) |
|
| Yes | - | Radiation is not coming from the front, nor is the person moving about in the field | Yes | Hp(0.07) |
|
| Yes | - | Radiation is not coming from the front, nor is the person moving about in the field | No, eyes preferentially exposed | Hp(0.07) |
|
Notes:
- Angle of incident radiation refers primarily to the angle of incidence between the radiation and the person. Angle and energy can have a large impact on the dosimeter’s response, and likewise have a large impact on whether Hp(10) or Hp(0.07) can be a surrogate for Hp(3).
- While the quantities Hp(10) and Hp(0.07) are both appropriate, since the body is non-uniformly exposed, the dosimeter should be worn close to the lens of the eye. Since extremity dosimeters are typically lighter and smaller than whole-body dosimeters, the extremity dosimeter type was selected here, keeping practicality in mind. (Extremity dosimeters by design measure Hp(0.07). A whole-body dosimeter that measures both Hp(10) and Hp(0.07) could be worn near the eye, if practical).
- The statement “the person is moving about in the field” indicates that the person is moving so that the radiation is not directed at the person from 1 or more dominant angles. If a person is largely side-on to or turned away from the source of radiation, the statement “radiation is not coming from the front nor is the person moving about in the field” would apply.
| Are protective eye shields used (protective eyewear)? | Does eye shield absorb beta radiation? | Operational quantity to be used | Recommended dosimeter type and placement |
|---|---|---|---|
| No | N/A | Hp(3) |
|
| Yes | No | Hp(3) |
|
| Yes | Yes | Not needed (eye dose nil) | Not needed (eye dose nil) |
Note: For beta radiation, if lead shielding is used, the possibility of the generation of bremsstrahlung – and of exposure to it – should be considered.
Appendix B: Assessing the Activity Handled for Selecting Participants in a Routine Intake Monitoring Program
B.1 Technical Basis
This appendix presents the technical basis for calculating the activity handled that triggers the need to participate in a routine bioassay program. The method outlined in this appendix is derived from the Health Physics Society publication ANSI/HPS N13.39–2001, Design of Internal Dosimetry Programs [28].
The principal parameter used for determining the activity of a substance above which routine bioassay should be undertaken is the potential intake fraction (PIF). It is a conservative estimate of anticipated intakes of a substance that could occur in 1 year. It assumes that intakes occur by the volatilization or re‑suspension of the substance with subsequent inhalation. It is a function of:
- the potential for the handled substance to become airborne
- the confinement used when handling the substance
- the substance’s dispersibility due to energy being added (e.g., heating)
- the occupancy time while handling the substance
- the affinity of the substance to bind to DNA once taken into the body
The PIF is defined as:
(21)
Where:
| 10-6 = | Brodsky’s factor |
|---|---|
| R = | release factor |
| C = | confinement factor |
| D = | dispersibility factor |
| O = | occupancy factor |
| S = | special form factor |
Brodsky’s factor is an empirical estimate of the fraction of material in a process that could be inhaled without considering the items in the bullet list above [28]. Each of the items in the bullet list is represented by one of the factors in equation 21. Default values for each factor are listed in table B.1 [28].
| Recommended values | ||
|---|---|---|
| Release factor (R) | Gases, strongly volatile liquids | 1.0 |
| Non-volatile powders, somewhat volatile liquids | 0.1 | |
| Liquids, general large area contamination | 0.01 | |
| Solids, spotty contamination, material trapped on large particles (e.g., resins) | 0.001 | |
| Encapsulated material | 0 | |
| Confinement factor (C) | Glovebox or hot cell | 0.01 |
| Enhanced fume hood (enclosed with open ports for arms) | 0.1 | |
| Fume hood | 1.0 | |
| Bagged or wrapped contaminated material, bagged material in wooden/cardboard boxes, greenhouses | 10 | |
| Open bench-top or surface contamination in a room with normal ventilation | 100 | |
| Dispersibility factor (D) | Actions that add energy to the material (heating, cutting, grinding, milling, welding, pressurizing, exothermic reactions) | 10 |
| Other actions (that do not enhance dispersibility) | 1 | |
| Occupancy factor (O) | Annual or one-time use | 1 |
| Monthly use or a few times per year | 10 | |
| Weekly, tens of times per year or tens of days for a one-time project | 50 | |
| Essentially daily use | 250 | |
| Special form factor (S) | DNA precursors (except 32P, 35S or 131I) | 10 |
| Other material | 1 | |
The occupancy factor is intended to reflect the number of times a radionuclide is handled in 1 year. It is not intended to be applied as a fraction of the total time that a worker may be exposed to a radionuclide and is therefore a unit-less quantity. In a case in which O = 1, the PIF would represent in this specific case the fraction of activity handled that could be inhaled from a single use. In situations in which handling is more frequent than once per year, O > 1, and the PIF represents the fraction of activity handled in 1 year that could potentially be inhaled.
The above formulation for the PIF may be modified to account for the protection afforded by respiratory protection equipment.
The values in table 6 in section 7.1.1 were derived from the following parameter values:
| Gases and volatile liquids |
R = 1 (gases, strongly volatile liquids) D = 1 (no energy added to system) O = 250 (essentially daily use) S = 1 |
|---|---|
| Powders |
R = 0.1 D = 1 (no energy added to system) O = 250 (essentially daily use) S = 1 |
| Non-volatile liquids and solids |
R = 0.01 (liquids, large area contamination) D = 1 (no energy added to system) O = 250 (essentially daily use) S = 1 |
B.2 Example: Determining Participation in a Bioassay Program
Work at a radiopharmacy involves the handling of I-123 and I-131. Work with these radionuclides may be carried out by the same person; therefore, both radionuclides are considered in the determination of whether the workers should be participating in a routine intake monitoring program and, if so, for which radionuclides.
1) I-123: At a facility, 1.1 GBq of I-123 are used twice per week to produce metaiodobenzylguanidine (mIBG) for patient doses. The process is carried out in a hot cell, and heating is applied as part of the procedure. The I-123 is initially in NaI form. The following parameters have been selected for NaI‑123:
R = 1 (gases, strongly volatile liquids)
C = 0.01 (hot cell)
D = 10 (actions that add energy to the material, e.g., heating)
O = 100 (weekly × 2)
A Te-121 impurity is known to be present in the stock solution (up to 3% of the total activity, i.e., 33 MBq). The above parameter values are applied to the Te-121 impurity as well.
The 1.1 GBq of NaI-123 are required to produce 850 MBq of I-123-mIBG. The parameter values for handling this latter type of compound are:
R = 0.1 (somewhat volatile liquids, to account for an unbound impurity)
C = 1 (fume hood)
D = 1 (other actions (that do not enhance dispersibility))
O = 100 (weekly × 2)
The activity remaining in the fume hood, 250 MBq, as NaI-123, is assigned the following parameter values:
R = 1 (gases, strongly volatile liquids)
C = 1 (fume hood)
D = 1 (other actions (that do not enhance dispersibility))
O = 100 (weekly × 2)
Weekly quality control (QC) checks are carried out on the product. These checks involve handling about 0.1 MBq I-123 as mIBG under a fume hood. The following parameters have been selected for this process:
R = 0.1 (non-volatile powders, somewhat volatile liquids)
C = 1 (fume hood)
D = 1 (other actions (that do not enhance dispersibility))
O = 50 (weekly)
In situations in which the release factor for a non-volatile compound is not known, R = 0.1 should be selected by default. Alternatively, a material-specific value for R may be used when available.
2) 111 GBq of I-131 in the form of NaI is handled once weekly for dispensing patient doses. Handling is carried out under a fume hood. The following parameters have been selected:
R = 1 (gases, strongly volatile liquids)
C = 1 (fume hood)
D = 1 (other actions (that do not enhance dispersibility))
O = 50 (weekly)
The following parameters are defined in section 7.1.1:
(22)
(23)
In the above expressions, Qj is the activity of radionuclide j handled daily (with specified confinement and release factors), PIFj is the potential intake fraction for the specified confinement and release factors, and ALIj is the annual limit on intake for radionuclide j.
The potential intake fraction is defined as PIF = 10-6 × R × C × D × O × S, where:
| R = | the release factor, a measure of the volatility of compounds. R may take values from 0 for encapsulated materials to 1 for gases and strongly volatile liquids. |
|---|---|
| C = | the confinement factor. Values of C vary from 0.01 for gloveboxes and hot cells to 100 to represent work on an open bench top. |
| D = | the dispersibility factor. For actions that add energy to the material (heating, cutting, grinding, milling, welding, pressurizing, exothermic reactions), D is assigned the value of 10. For all other actions that do not enhance dispersibility, D is assigned the value of 1. |
| O = | the occupancy factor, which reflects the frequency with which the activity Q is handled in 1 year. The product Q × O is the activity handled per year (Bq/year). |
| S = | the special form factor, which accounts for the risk associated with intakes of some DNA precursors. S is assigned a value of 10 for radionuclides bound to DNA precursors, with the exception of P-32, S-35 and I-131. For these radionuclides, and for all compounds other than DNA precursors, S is assigned a value of 1. |
As indicated in section 7.1.1, routine individual intake monitoring should be carried out for workers whose value of BT ≥ 1. Furthermore, when BT ≥ 1, routine individual intake monitoring should be carried out for radionuclides whose value of rj ≥ 0.3.
The rj values for I-123 and I-131 in this example are shown in table B.2. The processes involving I-123 consist of only 2 items. Consequently, an I-123-specific value of rj is calculated as indicated below. The parameters Qa and Qb represent the I-123 activity handled per day of use for each of the processes involving I-123.
(24)
For all processes that involve handling radioiodines in this case, BT = 111. Since BT > 1, individual intake monitoring at the facility should be carried out. Because rj = 111 for I-131, the facility carries out routine thyroid monitoring for I-131. For I-123, the value of rj » 0.01. Consequently, routine intake monitoring for I-123 is not carried out at this facility.
| Protocol | mIBG production | NaI dispensing | ||||
|---|---|---|---|---|---|---|
| Radionuclide | 123I | 121Te | 131I | |||
| Form | mIBG | NaI | mIBG | NaI | NaI | NaI |
| Use description | Weekly QC checks | Remaining NaI handled in fume hood | mIBG handled in fume hood | NaI stock solution in hot cell | Impurity in stock solution (3% of total initial activity) | Stock used for dispensing |
| Activity per use (Qi) MBq | 0.1 | 250 | 850 | 1,100 | 33 | 111,000 |
| R | 0.1 | 1 | 0.1 | 1 | 1 | 1 |
| C | 1 | 1 | 1 | 0.01 | 0.01 | 1 |
| D | 1 | 1 | 1 | 10 | 10 | 1 |
| O | 50 | 100 | 100 | 100 | 100 | 50 |
| PIFi | 5×10-6 | 1×10-4 | 1×10-5 | 1×10-5 | 1×10-5 | 5×10-5 |
| e(50) Sv/Bq | 2.1×10-10 | 2.1×10-10 | 2.1×10-10 | 2.1×10-10 | 3.9×10-10 | 2.0×10-8 |
| ALI Bq | 9.5×107 | 9.5×107 | 9.5×107 | 9.5×107 | 5.1×107 | 1.0×106 |
| rj |
0.01 |
1.3×10-4 | 111 | |||
Appendix C: Bioassay Protocols for Responding to Abnormal Intakes of Radionuclides
C.1 Introduction
This appendix describes 2 bioassay protocols that may be used by CNSC licensees to respond to situations in which persons may have experienced an abnormal intake of radioactive material. It also provides advice on how to collect and handle bioassay samples.
Sections C.6 and C.7 describe 2 response protocols involving the conduct of non-routine bioassays that may be used by CNSC licensees to ascertain the radiation dose to individuals when an abnormal intake of a radionuclide is known or suspected to have occurred.
C.2 Bioassay Methods
The radiation protection programs that the RPR require of CNSC licensees typically include provisions for bioassays. These bioassays may be “direct” or “indirect”.
A direct (or in vivo) bioassay is a measurement on the human body for the purpose of determining the amount of radioactive material in the body, utilizing instrumentation that detects the radiation emitted from the radioactive material.
An indirect (or in vitro) bioassay consists of the collection and analysis of a sample of human hair, tissue, blood, urine or feces for the purpose of determining the amount of radioactive material that might have been taken into the body.
C.3 Routine and Non-Routine Bioassays
Direct and indirect bioassays to ascertain radiation doses may be further characterized as “routine” or “non-routine,” as follows:
- A routine bioassay is any bioassay that involves collecting and analyzing samples or taking measurements on the body at scheduled intervals, or at predetermined times, during normal operations.
- A non-routine bioassay is any bioassay that is implemented as part of an ad hoc response to a particular circumstance, such as a known or suspected intake of radioactive material due to an abnormal incident in the workplace. Non-routine bioassays are often termed “ad hoc” or “special” bioassays.
By definition, a dose monitoring program that includes routine bioassays is proactive and precautionary in nature. Typically, such a program is intended to provide routine and timely detection, measurement and confirmation of any radioactive intakes that occur on an ongoing basis during normal operations. An example of a routine bioassay is the submission of a biweekly (every 14 days) urine sample for analysis for the presence of tritiated water.
A monitoring program that consists only of non-routine bioassays is typically reactive and ad hoc in nature. Such a program is usually custom-designed for the purpose of obtaining key parameters that are necessary in order to conduct a specific dose assessment in response to a specific, identified need. To avoid prejudicing the results, a non-routine bioassay is typically performed with the subject individual removed from further contact with, or exposure to, radioactive substances.
C.4 Selecting and Applying Bioassay Methods
In situations in which response protocols involving non-routine bioassays are implemented, the associated program for conducting bioassays and analyses will typically depend on case-specific factors, including:
- the time of intake of the radioactive contaminant(s)
- the mode of intake of the radioactive contaminant(s)
- the preliminary assessment of the radioactive intake and resulting dose, using the precipitating bioassay result and default parameters
- whether the radiation is due to a single radionuclide or a mixture of radionuclides
- the chemical and physical forms (e.g., particle size) of the radioactive contaminant(s)
- the types and energy of the radiation emitted by the contaminant(s)
- the rate of decay of the radioactive contaminant(s)
- the metabolic characteristics and behaviour of each suspected radioactive contaminant (e.g., retention time within the body, solubility within the body, rate of excretion from the body)
- when the bioassay results are expected to be available
- the number of bioassay results required
- the convenience, sensitivity, quality and suitability of the available bioassay equipment and facilities
The bioassay methods that are most often used to assess radiation doses from internal sources are in vivo counting and the analysis of collected samples of excreta, such as urine and feces. These methods are appropriate to a variety of situations. For example, bioassays of excreta may be the only reasonable option in a situation that involves radionuclides with no gamma-ray emissions or only low-energy photon emissions. Conversely, if a person may have been internally exposed to a mixture of radionuclides that emit penetrating gamma photons, a combination of in vivo counting and the collection and analysis of excreta may be appropriate.
In certain situations in which a standard bioassay method, or a combination of such methods, does not suffice to detect all radionuclides of concern, it may still be possible to use the method or combination of methods in conjunction with other knowledge or information to identify and estimate the impact of all radionuclides of concern. For example, where standard methods indicate the presence of certain radionuclides, it may be reasonable to conclude that certain other radionuclides, that is, those that are known to be normally associated with the radionuclides detected by the standard methods, are also present. The routine association, in irradiated uranium fuel, of fission product gamma emitters (detectable by in vivo counting or gamma spectroscopy on fecal samples using germanium detectors) with certain transuranic radionuclides is an example of such a situation. Accordingly, when a standard bioassay method detects a surrogate radionuclide, that discovery in light of the known or typical association of the surrogate with other radionuclides may indicate that associated radionuclides that can only be detected by some supplementary in vivo counting techniques or special analyses (e.g., fission track analysis for Pu‑239 in urine) are also present.
In addition, relevant metabolic data – such as organ or whole-body retention times, and urine and fecal excretion rates – can often be used (with appropriate adjustments) along with the results of bioassays to help ascertain the radiation exposures and doses from radioactive intakes.
C.5 Response Protocols
The response protocols recommended in this section are intended to be used following suspected or actual intakes of significant quantities of radionuclides. Such intakes typically occur during abnormal incidents in the workplace, such as those involving:
- the breach or failure of a sealed source
- the handling of unsealed radioactive sources
- airborne contamination as a consequence of fires or explosions
- the failure of personnel protection measures, such as respiratory equipment, during the maintenance or servicing of contaminated equipment or systems
An abnormal incident that occurs at a CNSC-licensed facility or during a CNSC-regulated activity could trigger a requirement (under applicable legislation, a CNSC licence or the licensee’s radiation protection program) for a non-routine bioassay.
In particular, when a licensee becomes aware that a dose to a person, an organ or a tissue may have exceeded an applicable dose limit prescribed by sections 13, 14 or 15 of the RPR, the licensee must conduct an investigation in order to determine the magnitude of the dose and establish the causes of the exposure (paragraph 16(c) of the RPR). The activities completed as part of the required investigation to determine the magnitude of the dose could include the conduct of a non-routine bioassay.
If the results of non-routine bioassays are to be credible, care should be given to such details as the choice and application of assay methods, the timing and number of in vivo counts, and the timing of the collection of excreta samples relative to the time of intake of radiation. Accordingly, persons who are responsible for designing and implementing response protocols should exercise competent judgment on key matters. For example, they should decide whether to collect and retain samples for confirmatory analyses, they should select appropriate times for truncation of sampling, and they should weigh and balance the associated advantages and disadvantages.
When selecting the preferred bioassay methods and identifying any complementary requirements for additional biological monitoring, the responsible persons should take into account the factors discussed in section C.4 above.
The response protocols that are described in section C.6 may be used to ascertain the CED resulting from an intake of radionuclides. However, users should exercise sound judgment. They should adjust and refine the recommended protocols to suit their specific needs and individual circumstances. These needs and circumstances will typically depend on case-specific factors, including radiation hazards in the workplace and the circumstances associated with the internal exposures.
It is recommended that, when feasible, material-specific data (e.g., solubility, particle size) be used over ICRP defaults in such evaluations because observed rates are typically more realistic than default values and thus more likely to result in a more realistic assessment of the associated radiation doses. An individual’s rate of retention or excretion cannot be adequately constructed on the basis of 2 or 3 randomly collected measurements or samples. Accordingly, these recommendations and protocols are designed to systematically yield case-specific bioassay data that are sufficient to generate scientifically defensible dose assessments.
The following situations would trigger the response protocols described in sections C.6 and C.7:
- A routine bioassay program yields an abnormal result, indicating that a person may have been exposed to abnormal levels of radiation.
- It is known or suspected that an abnormal incident has occurred (e.g., an initiating event such as a fire, an explosion or a failure of a ventilation system) that has a recognized potential to give rise to significant intakes of radionuclides by an affected person.
C.6 Response Protocol Triggered by a Routine Bioassay
As the first phase of this recommended response protocol:
- remove the exposed individual from any possibility of further intake
- confirm the initial bioassay result as soon as practical, using the laboratory that performed the analysis
- perform preliminary assessments of intake and dose using the results of the initial bioassays, taking factors such as those presented in section C.4 into account
- if the initial result is unusually high (e.g., much greater than an investigation level or approaching an effective dose limit for NEWs), consider confirming it with a laboratory that is independent of the laboratory that obtained the initial result
- where possible, when routine bioassays of a sample yield elevated results, retain the precipitating sample until all investigations associated with the incident are complete
Typically, samples can be most conveniently retained for use in repeat or additional analyses when only a small portion of the total collection is required for each analysis. For example, each determination of tritium in tritiated water in urine typically requires only 1 to 5 ml of urine, whereas the typical volume of a urine sample may range from 0.1 L to 1 L. Accordingly, a relatively small sample of urine, which occupies commensurate storage space, is sufficient for several tritium analyses.
Where practical, the unused portions of a urine or fecal sample should be retained for further analysis. For example, when non-destructive gamma spectroscopy of a feces sample indicates significantly elevated levels of fission and activation products, it may be both practical and prudent to reduce the sample to ash, and to save a portion of the ash for further analyses. In a few situations, it might be worthwhile to retain the unused portion of a sample until such time as improvements in analytical techniques or equipment give rise to more sensitive, accurate or reliable results.
As part of this protocol, non-routine sampling and bioassays are required in response to a routine bioassay that indicates that a worker has received a dose that exceeds a regulatory limit.
To be effective, a follow-up program of non-routine bioassays should take relevant factors into account. These factors include the considerations discussed in section C.4, the sampling and counting recommendations in table C.1, the radiation protection program, and the characteristics of the radionuclides involved.
Table C.1 recommends biological sampling and in vivo counting campaigns for 3 contiguous time periods (“1–10 days,” “10–100 days,” and “More than100 days”). The recommendations of table C.1 cover the time period during which the exposed person is removed from further work involving radiation or radioactive substances in the workplace.
Table C.1 addresses many, but not all, situations that are likely to be encountered by CNSC licensees. For example, where short-lived radionuclides (i.e., less than 3 days) are of concern, the time that is available for the purpose of conducting effective sampling will be commensurately short, and consequently, the sampling regime recommended in table C.1 may not be entirely appropriate. Similarly, the recommendations of table C.1 may not be entirely appropriate in situations in which long-lived radionuclides are incorporated into compounds that have short half-lives (less than 3 days). For such situations, sampling should be carried out daily during the 10 days that immediately follow intake in order to accurately define the shapes of the individual’s retention or excretion curves.
Where the results of a routine bioassay indicate that a worker’s intake may exceed an investigation level (IL), arrangements for the non-routine sampling and bioassays recommended in table C.1 should be made. It may also be appropriate to plan for any supplementary biological samplings (e.g., of blood, saliva or breath) as well as for bioassays that are required by the applicable radiation protection program or necessary in order to generate or improve estimates of intake or doses. For example, when an estimated dose exceeds 100 mSv, collection of blood samples for chromosomal analyses should be considered.
C.7 Response Protocol Triggered by an Abnormal Incident
This protocol is intended to be implemented in response to abnormal incidents in the workplace, such as accidents involving fires, explosions, failure of ventilation systems or failures of protective equipment. Abnormal incidents typically increase the levels of airborne radioactivity and can result in increased intakes. In addition, abnormal incidents that result in skin wetting by tritiated water can also result in increased intakes of radioactive material.
Because incidents such as fires, explosions or ventilation failures may be self-evident or typically trigger alarms or monitors, their times of occurrence are usually well known. In such a case, the time of any associated intake of radioactive contaminants by workers can typically be established with similar accuracy.
Following an abnormal incident at a nuclear facility, an increased intake by workers may be suspected from indirect evidence. For example, the detection of facial or nasal contamination by portal monitors or hand-held detectors, the presence of surface cuts or sores that are radioactively contaminated, or the presence of tritiated water on skin may indicate that the individuals have been subjected to an unplanned intake. Such evidence can be sufficient reason to immediately initiate a non-routine bioassay instead of awaiting the results of routine bioassay monitoring.
Where an intake of radioactive contaminants is suspected but not confirmed, the timely collection of non‑bioassay and bioassay samples may help establish whether or not such an incident has occurred.
Non-bioassay samples include swabs of nasal fluid and surface wipes of protective clothing or workplace surfaces. Either the presence of radionuclides in such media or the lack thereof can serve as a reasonable indicator of whether an inhalation incident has occurred.
In such cases, samples should be collected, results confirmed and doses ascertained as follows:
- Arrangements should be made for the timely collection of bioassay samples from the exposed individuals and the timely completion of in vivo counting, since the initial results of the bioassay or in vivo monitoring will influence decisions about further sampling. In cases of suspect tritium intakes, the bladder should be voided prior to bioassay sample collection.
- If widespread contamination is present, particular care should be taken to obtain uncontaminated bioassay samples (see section C.8).
- While awaiting the results of the initial bioassay sampling and the initial in vivo monitoring, sampling should continue at the frequencies recommended in table C.1.
- The results of the initial in vitro bioassay or in vivo counting should be reviewed and compared with the results of the available non-bioassay samples, such as nasal swabs or surface contamination wipe samples.
- If the radionuclides detected in the nasal swab and workplace wipe samples are the same as those reported in the bioassay results, this agreement should be considered to be confirmation that a corresponding intake has occurred.
- Preliminary assessments of intake and dose should be carried out using the results of the initial bioassay results, taking factors such as those presented in section C.4 into account.
Possible responses to the preliminary assessments of intake and dose are shown below:
- If the estimated intake or dose is less than the relevant IL, the protocols recommended in table C.1 may be adjusted accordingly. Since the intake is relatively low, it is appropriate to consider ending sampling much sooner than recommended in the table.
- If the estimated intake or dose is equal to or greater than the relevant IL, the protocols recommended in table C.1 should be followed. If appropriate, arrangements for additional specialized analyses and biological monitoring, as discussed in sections C.4 and C.5, respectively, should be made (for example, collecting blood samples for chromosomal analyses when the dose exceeds 100 mSv).
C.8 Collecting and Handling Bioassay Samples
C.8.1 General recommendations
- All persons who handle bioassay samples should be properly instructed in the safe handling of biological and radioactive specimens.
- The services of a qualified medical agency or practitioner to collect blood samples should be used.
- Sample collection in restricted zones should be carried out in areas where the probabilities of contamination of the samples are lowest.
- All samples should be collected in sterile disposable containers.
- When a fecal sample is required from a subject, the subject should be instructed to exercise caution to avoid contaminating the required sample with urine.
- After collecting a sample in a potentially contaminated workplace, showering or handwashing should be done before removing the samples to an unrestricted area.
- Where possible, all samples collected should be retained until all investigations associated with the incident are complete.
- When transporting bioassay samples, measures should be taken to preserve the integrity of the sample and to prevent damage, loss of radioactivity, or contamination of the samples.
C.8.2 Labelling samples
After collecting a bioassay sample from a person, the sample container should be labelled with the name or identification number of the person and the date and time of sample collection.
C.8.3 Treating and storing urine samples
If the urine sample is to be retained for more than 24 hours before it is analyzed, it should be placed in cold storage (such as in a refrigerator or cooler) immediately following its collection.
If a urine sample is to be retained for a significant or indeterminate period of time before it is analyzed, the sample should be treated to prevent or minimize bacterial growth or radionuclide losses to the walls of the sample container immediately following collection of the sample. Measures that are appropriate to the situation should be used, taking into account the characteristics and chemical forms of the radionuclides present in the sample. Typical approaches include adding acid to certain types of samples to prevent precipitation, or adding a preservative such as thymol to minimize bacterial growth.
Where appropriate, urine samples may be preserved by freezing. Freezing may be particularly appropriate and convenient for urine samples containing organically bound tritium, particularly those that may require a repeat or confirmatory analysis to determine the organically bound tritium present in the sample. Where possible, part of the collected samples should be retained for repeat or multiple analyses.
C.8.4 Collecting and storing fecal samples
When collecting fecal samples, specialty kits (e.g., a “commode specimen collection system”) that are designed for the purpose and readily available from commercial medical equipment suppliers should be used. Fecal samples that are not to be analyzed immediately should be frozen as soon as they are received.
| Period after intake | Urine sampling frequency | Fecal sampling frequency | In vivo count frequency | Comments |
|---|---|---|---|---|
| 1–10 days | A 24-hour urine sample should be collected each day. | A 24-hour fecal sample should be collected each day. | In vivo counting should be performed each day. | Sampling and/or in vivo counting may end when results fall below detection limits or reach chronic baseline values. |
| 10–100 days | A 24-hour urine sample should be collected every 14 days. | 24-hour fecal samples should be collected on 3 consecutive days. The collection program should be repeated every 14 days. | In vivo counting should be performed every 14 days. | Sampling and/or in vivo counting may end when results fall below detection limits or reach chronic baseline values. |
| More than 100 days | A 24-hour urine sample should be collected every 30 days. | 24-hour fecal samples should be collected on 3 consecutive days. The collection program should be repeated every 30 days. | In vivo counting should be performed every 30 days. | Sampling and/or in vivo counting may end when results fall below detection limits or reach chronic baseline values. |
Notes:
- The bioassay schedule recommended in table C.1 should typically be followed until the subject returns to work. However, users may modify the protocol to take into account individual circumstances. For example, the 3 discrete sampling periods shown in this table may not be appropriate for radionuclides with half-lives < 3 days, for long-lived radionuclides in chemical form that have biological half-lives < 3 days, or when the intake is above a detection limit but below an action level.
- In table C.1 a 24-hour sample is a sample integrated over a contiguous 24-hour period.
Appendix D: Radionuclide-Specific Recommendations Related to Bioassay Measurements and Internal Dosimetry – Tritium
D.1 Analytical Methods for Tritium in Urine
Tritium in urine is most readily assessed by liquid scintillation counting (LSC) of a urine sample. This method involves adding an aliquot of the urine sample to an organic liquid scintillator. Light photons, emitted by the scintillator as it absorbs beta particle energy, are detected by photomultiplier tubes operating in coincidence.
Because tritium is a low-energy beta emitter it may be necessary to correct for other beta emitters in a sample. Consequently, it is important to have a good knowledge of the beta-emitting radionuclides that may be present in the workplace. In order to take these interfering radionuclides into consideration, energy discrimination regions may be set on the LSC system. For example, energy discrimination regions may be selected in the ranges 0 to 18.6 keV for H-3, 35 to 110 keV for C-14, and 180 to 2,000 keV for other beta-emitting radionuclides. Regions should be selected so as to optimize the detection efficiency for counting urine samples.
The LSC system’s energy windows should be set using an unquenched standard (as quality control to verify the instrument stability). This setting should also be verified periodically. Because chemical and colour quenching from materials in the sample influence the counting efficiency, and because these factors vary from one sample to another, the assumed efficiency should be based on the characteristics of each sample. Most LSCs have an automatic quench correction mechanism. When this is not the case, a quench calibration curve should be established in order to determine the efficiency. The efficiency for each energy region should be calibrated using traceable standards under various quench conditions.
In addition, volumetric dispensers should be verified periodically and corrections made if the variation exceeds ± 10%. Periodic verification of the system performance should be carried out.
Sample preparation should be carried out under a fume hood. An aliquot of the sample and LSC cocktail are dispensed into an LSC vial and mixed thoroughly. Traceability checks should be used to ensure reliable sample identification. The activity measured in the low-energy region may be corrected to account for the low energy contributions from the higher energy beta particles if such higher energy beta‑emitting radionuclides are present.
D.2 Monitoring Frequency
Doses to workers from chronic intakes of tritiated water, or tritiated compounds that partially convert to hydrogenated tritium oxide (HTO) in the body (e.g., elemental tritium gas (HT)), should be ascertained by linear interpolation between successive routine bioassay measurements.
A monitoring period of 14 days or less is recommended when calculating the dose using the linear approximation method since this results in the error on the dose being less than 50%. When bioassay results exceed 1 MBq/L, monitoring should be carried out weekly until the concentration returns below that value [31].
A monitoring period longer than 14 days may be selected for workers with a low probability on HTO intakes; however, this monitoring period should not exceed 30 days. At such monitoring intervals, the condition expressed by equation 10 is satisfied for HTO.
It should be noted that when the HTO in urine concentration remains below 45 kBq/L, the annual CED remains below 1
mSv. Workers whose HTO in urine concentration is 45 kBq/L or more should submit routine urine samples at least
monthly. When the IL is exceeded and the intake is known to be acute in nature, the linear approximation method
should be replaced by the acute intake method described in section 9. Those individuals not submitting
routine urine samples should submit a urine sample for tritium analysis when exposures to HTO may exceed 10
DAC-hours. The DAC for HTO should be calculated by reducing the DAC for inhalation of tritiated water only by a
factor of 1.5 to account for absorption of tritiated water through intact skin. Based on the DAC definition
(equation 7), the DAC for tritiated water is DACHTO = 3 × 105 Bq/m3.
In special bioassay monitoring, because the concentration of HTO in body water reaches a maximum a few hours after an acute intake, sampling should account for dilution of HTO with the existing bladder contents.
D.3 Ascertaining Dose
When routine bioassay is carried out and no significant acute intake is suspected (i.e., when special bioassay monitoring is not initiated), the CED (in Sv) resulting from tritium intakes during a reporting period (e.g., 1 quarter or 1 year) should be ascertained using the method illustrated below. This method should be used for intakes of HTO and HT.
The accumulated dose, Ek, received during the reporting period k, should be calculated from a series of N measurements of tritium in urine made during period k, as shown below [31].
(25)
Here, Ci is the concentration of tritiated water in urine, in units of Bq/L, measured at time ti days. The concentration C0 is the result of the last concentration measurement made in the reporting period previous to period k.
The CED, that is, the effective dose received from HTO in the body for 50 years following intake, from the end of reporting period k, is Ek(50). It should be calculated as follows.
(26)
The CED for a dosimetry year is the sum of all Ek values for the year and Ek(50). In figure D.1, ta is a reporting time, and the dose reported at ta is the accumulated dose to time t1, as well as the dose between t1 and ta (calculated assuming the biological half-life of HTO to be 10 days). The dose accumulated between ta and tb may be calculated as follows:
(27)
.png/object)
It should be noted that a licensee may propose other formulations that provide an equivalent approximation for the effective dose accumulated during a monitoring period as per equation 27. Furthermore, licensees may ascertain the CED from tritiated water intakes by applying equation 26 instead of equation 25 for workers who have been absent from the workplace for an extended period of time (e.g., for more than 60 days).
D.4 Quality Control of Liquid Scintillation Counters
The performance of LSC used for measurements of tritium in urine should be verified each day it is in use. Verifications should also be carried out following the installation or servicing of a liquid scintillation counter and after any event that may influence its accuracy. The information shown in table D.1 should be recorded as part of the quality control program. These data should also be recorded graphically on control charts.
Table D.1: LSC performance log
| Source | Number | Activity (dpm) | Date |
|---|---|---|---|
| Background | |||
| Tritium | |||
| Carbon-14 |
| Channel | Gain | Low level | High level |
|---|---|---|---|
| 1 | |||
| 2 | |||
| 3 |
| Date | Count time (min) | Count rate (cpm) | Comments | Operator’s initials | |||
|---|---|---|---|---|---|---|---|
| Background source | Check source | Background source | H-3 source | C-14 source | |||
The check sources used for verifying the counter performance should be flame-sealed. They should be used for no more than 5 years after sealing. The check source should be counted daily, long enough to accumulate at least 20,000 counts. The minimum counting time should be 30 seconds and the same counting time should be used for each measurement. In addition to a flame-sealed check source, a flame‑sealed background source is recommended and should be counted twice per day. The count time for the background checks should not change.
The standard deviation of the check source and background count rates should be calculated monthly. The check source and background count rates should be plotted on a control chart. Control limits at 2 standard deviations should be placed on the control chart. About 95% of the daily check source count rates should lie within the 2 standard deviation control limits. If either a daily check source or a background count rate is outside the control limits, the measurement should be repeated. If the second measurement is also outside the control limits, the instrument settings should be verified.
Appendix E: Radionuclide-Specific Recommendations Related to Bioassay Measurements and Internal Dosimetry – Radioiodines
This appendix provides guidance to licensees with respect to developing a thyroid screening program for radioiodines. It has been written mainly as guidance to supplement licence conditions for the use of nuclear substances.
This appendix includes recommendations on participant selection for the screening program, instrument selection, screening method, monitoring periods, interpretation of results, validation procedures, and record keeping. It considers iodine-123, iodine-124, iodine-125 and iodine-131; however, the approach may also be applied to other radioiodines.
E.1 Background
The purpose of a thyroid screening program is to monitor workers for intakes of radioiodines. Timely information produced by the program should be used to assess any intake of radioiodines, provide assurance that the radiation protection program is working, and demonstrate compliance with regulatory dose limits.
In a thyroid screening program, workers are individually monitoring for intakes of radioiodines by in vivo counting of the thyroid. Results are compared with a predetermined level. If the predetermined level is exceeded, confirmation of intake and an investigation are required. The licence conditions regarding thyroid monitoring depend on the physical characteristics of the radioiodine handled. Physical characteristics of the 4 radioiodines considered in this appendix are shown in table E.1 [14, 25, 35].
| Characteristics | 123I | 124I | 125I | 131I |
|---|---|---|---|---|
| Physical half-life (days) | 0.55 | 4.176 | 59.40 | 8.02 |
| Effective half-life in the thyroid (days) | 0.55 | 3.97 | 34.09 | 7.29 |
| Time to maximum thyroid burden after acute exposure Footnote 9 (days) | 0.5 | 1.1 | 1.9 | 1.3 |
| Main photon energy (keV) | 158.97 | 602.7 | 27.0 | 364.5 |
E.2 Participant Screening
E.2.1 Workers – Normal handling
Workers (NEWs and persons who are not NEWs) who handle a total quantity of radioiodine in 1 day that exceeds the amounts indicated in table E.2 should be screened for I-123, I-124, I-125 or I-131, as applicable. Examples of volatile radioiodine compounds can be found in section E.7. That section also describes actions that may generate such compounds.
| Confinement | ||||
|---|---|---|---|---|
| None | Fume hood | Glovebox | ||
| Quantity of 125I or 131I (MBq)) | Gases, volatile liquids and powders | 2 | 200 | 20,000 |
| Non-volatile liquids and solids | 200 | 20,000 | 2 × 106 | |
| Quantity of 124I (MBq)) | Gases, volatile liquids and powders | 3 | 300 | 30,000 |
| Non-volatile liquids and solids | 300 | 30,000 | 3 × 106 | |
| Quantity of 123I (MBq)) | Gases, volatile liquids and powders | 200 | 20,000 | 2 × 106 |
| Non-volatile liquids and solids | 20,000 | 2 ×106 | 2 × 108 | |
Other persons who regularly work close to a worker handling more than the amounts in table E.2 without confinement should also be screened for the relevant radioiodine. The values in table E.2 may be modified to account for the protection afforded by respiratory protection equipment.
E.2.2 Screening in response to spills and personnel contamination
Workers and other persons who have been in proximity to a spill, as described by one of the following situations, should be screened for the relevant radioiodine:
- involved in a spill of I-125 or I-131 in volatile form, where the activity exceeds 2 MBq
- involved in a spill of I-124 in volatile form, where the activity exceeds 3 MBq
- involved in a spill of I-123 in volatile form, where the activity exceeds 200 MBq
- externally contaminated by a volatile radioiodine
It is important that thyroid screening be completed as soon as possible after a spill or upset condition in which there is the potential for an internal exposure. Prompt initial thyroid screening will ensure that radioiodine intakes are detected and that actions can be taken, as appropriate, to minimize the worker’s CED through the administration of an iodine thyroid blocking agent. Completing thyroid screening less than 1 hour after an upset condition may be too early to detect a CED of 1 mSv or less; however, it would enable the early detection of a significant intake. In the first few hours following exposure, administration of an iodine thyroid blocking agent can be very effective at blocking the uptake of radioiodine by the thyroid. However, the effectiveness diminishes significantly as the time between the intake and the administration of the agent increases. After 24 hours post-exposure, the usefulness of iodine thyroid blocking is negligible.
Guidance on responding to personnel contamination can be found in REGDOC-2.7.1 [1]. Other approaches for responding to spills of radioiodines may be submitted to the CNSC for review and acceptance.
E.3 Instrument Selection
The scintillation detector is currently the most common type of instrument used for measuring radioiodine in the thyroid. It typically consists of a probe (usually containing a sodium iodide (NaI) crystal) operated in conjunction with a counter and a spectrum analyzer.
Systems can be as simple as a portable unit that produces results in counts per unit time, or as sophisticated as a gamma spectroscopy system that generates the energy spectrum of the isotope and then quantifies the total activity. Information on selecting a detector for I-125 or I-131 may be found in a number of references, such as in the Canadian Journal of Medical Radiation Technology article titled “Thyroid Monitoring Part VI: Choosing a Detector for Either I-125 and/or I-131” [32].
The NaI detector comes in various sizes and configurations depending on the desired use and sensitivity. When choosing a NaI detector, licensees should consider:
- the gamma energy of the radioiodine isotope to be measured
- the thickness of the NaI crystal
- the diameter of the NaI crystal
- the window material and configuration of the probe
E.3.1 Crystal thickness
The thickness of the NaI crystal required varies depending on the isotope of radioiodine being measured.
Detection and measurement of I-125 requires only a thin crystal to efficiently detect low-energy I-125 photons. Typically, NaI crystals approximately 1 mm thick are used to measure low-energy photon emitters such as I-125.
Conversely, a thicker crystal is required for the efficient detection of higher energy photons, from I-124 or I-131 for example. A crystal approximately 25 mm thick is recommended in these cases.
Given the similarity in the energies of the gamma radiation emitted, the detector used for measurements of I-125 (thin crystal NaI) may be used for the detection and measurement of I-123. Similarly, the detector used for measurements of I-131 (thick crystal NaI) may be used for the detection and measurement of both I-123 and I-124.
E.3.2 Crystal diameter
Another factor to consider is the diameter of the crystal. A large diameter results in greater overall counting efficiency. It also helps reduce errors that may result from any variances such as neck‑to‑detector distances, misalignment of detector with thyroid, and size of thyroid. However, a larger detector diameter increases the background reading.
Window material of probe
The window material of the probe is also a factor to be considered. The low-energy I-125 photons require a window material, such as Mylar or beryllium that is thin enough to allow the I-125 photons to penetrate the crystal.
If a probe is required to detect both I-125 and I-131, the crystal should be thick enough to detect I-131 and the window material thin enough to allow penetration of I-125.
Table E.3 summarizes the recommended specifications for detector uses to measure isotopes of iodine.
| Specification | 125I | 123I, 124I, 131I |
|---|---|---|
| Minimum crystal thickness (mm) | 1 | 25 |
| Minimum crystal diameter (mm) | 25 | 25 |
| Typical window material of probe | Mylar or beryllium | Aluminum or stainless steel |
| Typical energy range of detector (keV) | 20–200 | ≥ 40 |
E.4 Screening Method
E.4.1 Set-up
To install a counting system:
- Set up the counting system in an area of low, or at least non-variable, background radiation.
- Ensure that the equipment is set up according to the manufacturer’s specifications.
- Determine the background count rate using a neck phantom (ideally containing potassium).
- Calibrate the system by following the procedure set out in section E.8.
- Calculate and record the count rate equivalent to 1 kBq and 10 kBq in the screening log (see section E.9 for a sample screening log).
- Verify the set-up every time the system or location is changed to confirm its adequacy or make appropriate modifications.
E.4.2 Quality control verifications
To verify the ambient background and the reproducibility of the system’s count rate, the following steps should be taken on each day that thyroid screening is conducted:
- Measure and record the background count rate, accumulating at least 400 counts.
- Measure and record the net count rate of a standard source.
- Record the background and standard source count rates so that deviations from the norm can be readily observed (see section E.10 for a method of recording count rates using control charts).
As a best practice, verify controls annually by participating in a thyroid intercomparison program such as the one provided by Health Canada and described in the Human Monitoring Laboratory technical report titled The Thyroid Intercomparison Program [33].
E.4.3 Screening measurement
To perform a screening measurement:
-
Measure the person’s background count rate:
- this may be done by taking the measurement on the person’s lower thigh: although a thigh measurement simulates iodine that might be in the circulatory system, it should be noted that some detection equipment does not allow thigh measurements; in addition, thigh measurements may be affected by contamination of clothes or skin.
- if it is not feasible to carry out a background measurement on the thigh, an alternative method of measuring the background is to use a neck phantom (ideally containing potassium); if the background measurement is higher than usual, verify for possible contamination and repeat the measurement if necessary.
- Record the reading in the screening log.
- Measure the person’s count rate resulting from the thyroid.
- Record the reading in the screening log.
- Compare the result with the investigation and reporting levels recorded in the screening log.
- Depending on the measurement results, take the appropriate action based on the options provided in section E.6 and complete the screening log.
E.5 Monitoring Period
Some CNSC licences stipulate the routine monitoring period for certain radioiodines, such as monitoring between 1 and 5 days after the last use of I-124, I-125 or I-131. In cases where the routine monitoring period is not specified in a licence condition, it should be selected based on the principles set out in section 7.1.5.
E.6 Validation of Screening Results
E.6.1 General level
For all screening measurement results of I-124, I-125 or I-131 equal to or greater than 1 kBq, or screening measurement results of I-123 equal to or greater than 10 kBq, the licensee should proceed as follows:
- Verify that the screening measurement method described in section E.4.3 has been followed.
- If necessary, make any corrections and repeat the measurement.
- If the measurement result is still equal to or greater than 1 kBq, check clothes or skin for contamination.
- If clothes or skin are contaminated, remove the clothes or decontaminate the skin and repeat the measurement.
- If the measurement result is still equal to or greater than 1 kBq, ascertain and record the committed effective dose, and follow the steps in sections E.6.2 or E.6.3, as applicable.
- Screen all persons who worked in proximity to the person whose results are equal to or greater than 1 kBq.
E.6.2 Investigation level
For all screening measurement results of I-124, I-125 or I-131 equal to or greater than 1 kBq and less than 10 kBq, or screening measurement results of I-123 equal to or greater than 100 kBq, the licensee should:
- validate the results as per section E.6.1
- perform an internal investigation to determine and correct the cause of the screening results
- record the findings
- correct any deficiencies found by the investigation
- record the event in the annual compliance report
E.6.3 Reporting level
For I-124, I-125 and I-131, a 10 kBq thyroid screening result is approximately equal to a committed effective dose of 1 mSv. This is also the case for an I-123 screening result of 100 kBq. Under section 16 of the RPR, the CNSC must be notified when a licensee becomes aware that a dose to a person may have exceeded an applicable dose limit. For NEWs, the effective dose from each component of the dose that contributes more than 1 mSv per year should be ascertained.
For all screening measurement results of I-124, I-125 or I-131 equal to or greater than 10 kBq, or of I-123 equal to or greater than 100 kBq, the licensee should:
- validate the results as per section E.6.1
- immediately inform the CNSC if the measurement was made on a person other than a NEW
- have a radioiodine bioassay performed by an organization that has passed the relevant Health Canada intercomparison test in the previous 12 months or, if such an organization is unavailable, seek CNSC approval to permit someone else to perform the radioiodine bioassay
- use the results of the bioassay to ascertain the committed effective dose
- perform an internal investigation to determine and correct the cause of the screening results, including area and contamination monitoring at the site of the radioiodine intake, if applicable
- record the event in the annual compliance report
E.6.4 Screening log
The licensee should maintain a thyroid screening log. An example is provided in section E.9.
E.7 Volatile Radioiodine Compounds
Volatile radioiodine compounds include such compounds as sodium iodide (NaI) and radioiodines in a disassociated form. The volatility of radioiodine compounds may increase as a result of acidifying or freezing.
Activities that may cause radioiodine to be released include opening stock reagent containers, opening packages containing capsules used for therapeutic or diagnostic purposes, and working with such open packages. Therefore, capsules given to patients for diagnostic tests or for therapeutic purposes are considered to contain radioiodine in volatile radioiodine form.
The addition of antioxidants, such as sodium thiosulfate, to either labelled or NaI solutions reduces both decomposition and volatility. Furthermore, maintaining radioiodine solutions at dilute concentrations minimizes radiolytic decomposition. It should also be noted that radioimmunoassay kits contain small quantities of I-125 in a non-volatile form.
E.8 Instrument Calibration
E.8.1 General
All equipment and instruments used for thyroid screening should be maintained in good operating condition and must be calibrated as per section 25 of the RPR. Calibration must be performed for the isotope of interest under conditions mimicking the thyroid in the neck. An example of a calibration procedure can be found in “Thyroid Monitoring Part III: A Basic Calibration Procedure for Thyroid Monitoring” [34]. Once set up (as per section E.4.1), the measurement equipment must be calibrated if a quality control measurement is outside the control limits, as described in section E.10. In addition, the measurement equipment must be recalibrated prior to being put back into service if it has undergone any significant changes, such as repair or replacement that may have an adverse impact on the precision, accuracy or reliability of the measurements.
E.8.2 Detector efficiency
To determine absolute detector efficiency, measure the activity of a traceable standard source of the isotope of interest and use the following formula:
(28)
Where:
| E = | the efficiency in counts per second (cps) per becquerel (Bq) |
|---|---|
| C = | the measured counts per unit time of the standard source, in cps |
| B = | the background count rate, in cps |
| A = | the known activity of the standard source, traceable to a national standardizing laboratory within 5% (2σ, or standard deviation) accuracy, in Bq./td> |
The licensee should ensure that if a short-lived standard source is used (e.g., I-131), the activity of the source is corrected for decay to the day on which the calibration is performed. Appropriate, longer-lived, surrogate standard sources include: Te-123m (for I-123), Cs-137 (for I-124), I-129 (for I-125) and Ba-133 (for I-131).
The instrument and measurement parameters used to determine counting efficiency should be the same as those used for routine screening. Placing the detector as close to the thyroid as possible achieves the greatest efficiency. However, because of variations in thyroid depth, size, shape and positioning, large uncertainties can be introduced into the activity estimate. Such errors can be reduced by increasing the distance between the neck and the detector. Each system has its own optimal compromise between high efficiency and error reduction, but generally a good neck-to-detector distance is 12 cm.
The licensee should ensure a long enough count time for both the standard source and the background count rate so that overall error (2σ) in the count is less than 5%. This means approximately 400 gross counts for the background measurement.
E.8.3 Minimum detectable activity
The licensee should conduct measurements to achieve a minimum detectable activity (MDA) that is less than 1 kBq. The MDA is described in section 7.2.5. When the sample and background count times are equal, the MDA formula shown in section 7.2.5 reduces to the formula below:
(29)
Where:
B = the total background counts collected during time T
E = the efficiency in cps/Bq
T = the time in seconds
Equation 29 applies when the subject and background count times are equal. When they are not equal, equation 11 should be used instead.
E.8.4 Sample MDA calculation
If a system’s MDA is not low enough – either because of a low efficiency or high background – it can be improved. This can be done by increasing the counting time used for the measurement, decreasing the background, or both.
As an example, consider I-125. Assuming that the efficiency is 0.0060 cps/Bq and the gross background count is 400 counts, a 300-second count time would result in the following MDA, using the equation in section E.8.3:
(30)
The resulting value, 53 Bq, is acceptable for I-125.
The counting time used to monitor personnel does not have to be as long as that used for calibration. In the example above, the background is 400 counts/300 seconds, or 1.3 cps. Assuming the background count rate is stable, a 60-second count time would result in approximately 80 counts. Substituting these new figures into the equation produces a new MDA value, as shown in the following formula:
(31)
E.8.5 Records
Accurate calibration and service records should be maintained for the measurement system. The records should contain the following information:
- calibration date
- reference method
- calibration source current activity
- background values (these should be compared with previous values to detect changes)
- MDA
- calculated efficiency
- authorization signature
E.9 Sample thyroid screening log for iodine‑131
Investigation level: ________________________ net cps = 1 kBq of I-131
Reporting level: >________________________ net cps = 10 kBq of I-131
Employee name: _______________________________________________
Instrument used: _______________________________________________
| Date of measurement |
Last use of radioiodine (date) |
Background count rate (cps) |
Gross counts |
Count time (seconds) |
Net count rate (cps) |
Technician (initials) |
Action taken |
|---|---|---|---|---|---|---|---|
E.10 Quality Control Charts
This section provides a method for recording background and standard source count rates for quality control verifications.
Prepare 2 control charts, one for each of the background and standard source quality control verifications described in section E.4.2. Each control chart should show the date that measurements were taken and the corresponding count rates. After approximately 20 days of counting operations, there will be enough observations to estimate the standard deviations for the distributions. The standard deviation can be estimated in the following equation:
(32)
Where:
S = the standard deviation
n = the number of either background or standard source measurements
Ni = the count rate of each individual measurement
= the average of n measurements of Ni
The licensee should draw control limits at ±2S on each chart. Nearly all the quality control measurements (95%) should lie within the control limits.
If a quality control measurement of the background or standard source is outside the control limits, repeat the measurement immediately. If the repeated measurement is also outside the limits, verify the instrument settings. Lastly, if no cause can be found, the licensee may need to take remedial action, including recalibrating or repairing the instruments to ensure that subsequent quality control measurements are within the control limits.
Appendix F: Radionuclide-Specific Recommendations Related to Bioassay Measurements and Internal Dosimetry – Uranium
F.1 Annual Limits on Intake of Uranium Compounds
Natural uranium contains 3 isotopes: U-234, U-235 and U-238. Their respective activities per gram of natural uranium are 12,430 Bq, 575.9 Bq and 12, 350Bq. The mass percentages are 99.2742%, 0.7204% and 0.0054% for U-238, U-235 and U-234, respectively, and the specific activity is 2.54 × 104 Bq g-1, as outlined in ICRP Publication 107, Nuclear Decay Data for Dosimetric Calculations [35], and in the National Institute of Standards and Technology’s Atomic Weights and Isotopic Compositions database [36]. This section presents guidance on the selection of appropriate annual limits on intake (ALIs) for various uranium compounds, including those that have been enriched or depleted in the U-235 content.
The committed effective dose per unit intake (dose coefficients) and the corresponding ALIs for the inhalation of uranium compounds should be calculated for the solubility characteristics of those compounds to which workers may be exposed in the workplace. When no such material-specific dose coefficients and ALIs are available, the values from table F.1 should be used. Data for table F.1 was sourced from CNSC-RSP-0297, Evaluation of Default Annual Limit on Intake (ALI) for Yellowcake and Uranium Ore [37].
| Uranium compound | Annual limit on intake (Bq) | ||
|---|---|---|---|
| Natural uranium | Enriched (3.5%) uranium | Depleted uranium | |
| Uranium ore | 4,500 | N/A | N/A |
| Dried yellowcake | 48,000 | N/A | N/A |
| Calcined yellowcake | 3,100 | N/A | N/A |
| ICRP default Type F | 32,400 | 31,300 | 33,600 |
| ICRP default Type M | 12,000 | 9,850 | 11,600 |
| ICRP default Type S | 3,190 | 3,010 | 3,390 |
Material-specific ALIs should be derived from in vitro solubility studies of the relevant compounds. The study methodology and results should be documented as part of the licensee’s dosimetry technical basis. The solubility study should be updated periodically to reflect changes in processes or types of compounds encountered at the licensed facility, or to verify that solubility parameters have not changed.
F.2 Chemical Toxicity of Uranium Compounds
Because uranium is a heavy metal, it is chemically toxic above a threshold concentration in the kidneys. Chemical toxicity should be considered when inhalation intakes of soluble uranium compounds, and intakes by ingestion as well as via wounds, are likely. In order to prevent uranium from affecting the kidneys, urine bioassay measurements should be used to verify that the concentration of uranium does not exceed the peak kidney burden. The peak kidney burden should be established between 0.3 to a maximum of 3 μg of uranium per gram of kidney tissue. For further information, consult ISO 16638-1, Radiological Protection – Monitoring and Internal Dosimetry for Specific Materials – Part 1: Inhalation of Uranium Compounds [38]. Table F.2 shows urinary concentrations resulting from a peak kidney burden of 3 μg of uranium per gram of kidney tissue. The concentrations are averages for the 24-hour period listed. For the time period of 1 day, the concentration is the average for the period from time 0 to 24 hours following the intake. Table F.3 provides the excretion rates and concentrations for smaller time intervals in the first 48 hours following an intake. Data for tables F.2 and F.3 was sourced from CNSC-RSP-0165, Uranium Intake – Dose Estimation Methods [39].
| Time post-intake (days) | Uranium in urine concentration µg/L | |||
|---|---|---|---|---|
| Type F | Type M | Type S | Ingestion | |
| 1 | 3,760 | 3,760 | 3,720 | 3,700 |
| 2 | 130 | 182 | 233 | 204 |
| 3 | 105 | 138 | 137 | 109 |
| 4 | 95 | 128 | 125 | 98 |
| 5 | 86 | 119 | 116 | 89 |
| 6 | 78 | 111 | 108 | 81 |
| 7 | 71 | 105 | 101 | 74 |
| 8 | 65 | 99 | 95 | 67 |
| 9 | 60 | 93 | 90 | 62 |
| 10 | 55 | 88 | 85 | 57 |
| 14 | 40 | 72 | 69 | 41 |
| 30 | 14 | 43 | 41 | 14 |
| Time post-intake (hours) | Type F | Type M | Type S | Ingestion | ||||
|---|---|---|---|---|---|---|---|---|
| µg U per 4 h | µg/L | µg U per 4 h | µg/L | µg U per 4 h | µg/L | µg U per 4 h | µg/L | |
| 4 | 3,100 | 13,300 | 2,600 | 11,100 | 1,310 | 5,620 | 819 | 3,510 |
| 8 | 1,330 | 5,690 | 1,430 | 6,150 | 1,680 | 7,220 | 1,850 | 7,930 |
| 12 | 477 | 2,040 | 659 | 2,830 | 1,120 | 4,780 | 1,290 | 5,530 |
| 16 | 202 | 865 | 319 | 1,368 | 609 | 2,611 | 696 | 2,982 |
| 20 | 99 | 423 | 164 | 702 | 318 | 1,363 | 351 | 1,504 |
| 24 | 57 | 245 | 93 | 400 | 170 | 728 | 178 | 761 |
| 28 | 40 | 171 | 61 | 263 | 99 | 422 | 96 | 410 |
| 32 | 33 | 140 | 47 | 201 | 65 | 278 | 58 | 249 |
| 36 | 29 | 126 | 40 | 173 | 49 | 210 | 41 | 176 |
| 40 | 28 | 119 | 37 | 159 | 41 | 177 | 33 | 142 |
| 44 | 27 | 115 | 35 | 151 | 37 | 160 | 30 | 127 |
| 48 | 26 | 112 | 34 | 147 | 35 | 151 | 28 | 119 |
When a worker’s urine monitoring result exceeds the applicable value from table F.2 or F.3, the worker should be removed from work involving soluble uranium compounds, and an additional urine sample should be obtained to confirm the initial result. If the intake is confirmed, the worker should be referred to medical personnel for a kidney function test.
The dominant mode of uranium toxicity depends on the compound solubility, the U-235 enrichment, and the presence of other uranium isotopes.
Chemical toxicity is limiting in the following conditions:
- acute inhalation intakes of Type F compounds of all U-235 enrichments
- acute inhalation intakes of Type M compounds of U-235 enrichments less than 30% by mass
- chronic inhalation intakes of Type F compounds of U-235 enrichments less than 3% by mass
Radiological toxicity is limiting in the following conditions:
- acute or chronic inhalation intakes of Type S compounds of any U-235 enrichment
- acute or chronic inhalation intakes of any absorption type when U-232 or U-236 is present
- chronic inhalation intakes of Type F compounds of U-235 enrichments of 3% or more by mass
- chronic inhalation intakes of Type M compounds of any U-235 enrichment
Chemical and radiological toxicity are equivalent for acute inhalation intakes of Type M compounds with U-235 enrichments of 30% or more by mass. In cases of intakes via a wound, the radiological and chemical toxicity should both be assessed on a case-by-case basis. For further information, consult ISO 16638-1, Radiological Protection – Monitoring and Internal Dosimetry for Specific Materials – Part 1: Inhalation of Uranium Compounds [38].
F.3 Ascertaining Dose From Intakes of Uranium Compounds
In addition to the recommendations in Part B of this regulatory document, the following should be considered when ascertaining the dose from intakes of uranium compounds.
F.3.1 In vitro bioassay
Measurements of uranium in urine samples should be used to:
- ascertain doses from intakes of soluble uranium compounds
- serve as an indicator of intakes for uranium compounds of any solubility
- verify that intakes calculated from air monitoring are representative of actual intakes
- supplement in vivo monitoring data in special bioassay monitoring to ascertain the dose
- verify the proper functioning of respiratory protective equipment
F.3.2 In vivo bioassay
In vivo bioassay monitoring for intakes of uranium consists of lung counting. The following should be considered when measuring uranium in the lungs.
Measurements of the chest wall thickness (CWT) should be carried out for every worker taking part in a lung counting program for uranium. The measurements may be made by ultrasound. The frequency of these measurements should be documented. Calibration of the ultrasound units used for CWT measurements should be documented and verified periodically. The CWT of every worker taking part in a lung counting program should be documented and updated periodically. Each worker’s CWT should be used in ascertaining their lung burden (e.g., mg of uranium) from the lung counting results.
Triggers for repeating lung counts should be established and documented. These should be based on considerations of surface contamination of counted workers. When surface contamination has been confirmed on a worker such that their lung count results are inaccurate, the worker should be asked to shower and then be recounted.
Appendix G: Radionuclide-Specific Recommendations Related to Air Monitoring and Internal Dosimetry – Radon progeny
G.1 Introduction
Radon is a naturally occurring radioactive noble gas. There exist several isotopes of radon; however, the most significant in terms of occupation dose is Rn-222, which is part of the U-238 decay chain. The majority of the dose from inhaled Rn-222 results from the decay of its short-lived progeny. The focus of this appendix is on ascertaining worker doses from inhaled Rn-222 and its short-lived progeny. Occupational intakes of other isotopes of radon, such as Rn-220, are not covered in this appendix because they do not contribute significantly to worker doses in modern Canadian uranium mines. Guidance on the topic, however, can be found in ICRP Publication 65, Protection Against Radon-222 at Home and at Work [40]. Figure G.1 shows the U-238 decay chain, and highlights the Rn-222 short-lived radioactive progeny.
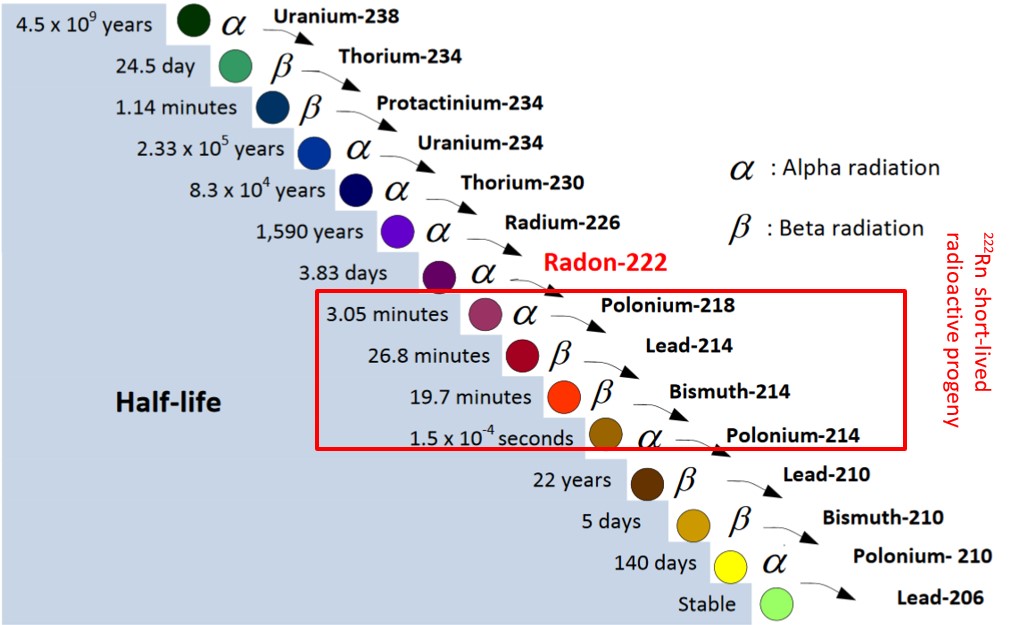
The potential alpha energy exposure (PAEE) is the time integral of the potential alpha energy concentration in air, to which an individual is exposed over a given time period. The potential alpha energy concentration is the concentration of short-lived Rn-222 progeny in air in terms of the alpha energy released during the complete decay through Po-214. The PAEE is expressed in working level months WLM and derived as described in section G.3.
G.2 Dose Coefficients for Radon Progeny
The effective dose conversion factors of 5 mSv/WLM for NEWs and 4 mSv/WLM for persons who are not NEWs are derived based on the detriment of radon progeny per unit effective dose, as defined by the ICRP 65[40]. For workers, this value is 5.6 × 10-5 Sv-1, and for the public it is 7.3 × 10-5 Sv-1 [41]. For both workers and the public, the detriment per PAEE is 2.83 × 10-4 WLM-1 [40]. The ratio of the detriment per PAEE to the detriment per unit effective dose results in the effective dose conversion factors.
To calculate the dose to NEWs, from their PAEE in WLM, which is calculated through air monitoring, the PAEE should be multiplied by 5 mSv/WLM to obtain the effective dose. To calculate the dose to persons who are not NEWs, from their PAEE in WLM, the PAEE should be multiplied by 4 mSv/WLM to obtain the effective dose.
G.3 Measuring the Concentration of Radon Progeny and Deriving the PAEE
A representative volume of air should be sampled to measure the airborne radon progeny concentration, either on an instantaneous or continuous basis. Instantaneous samples are typically those collected over short intervals of a few minutes. Continuous samples are those collected over much longer time intervals, typically hours or days.
One radon progeny measurement approach acceptable to the CNSC is the modified Kusnetz method. It consists of:
- filtering a representative volume of air to collect a sample of airborne radon progeny
- measuring the alpha emissions that occur during radioactive decay of the collected progeny
- using observed, measured and known data, and established formulae, to estimate the atmospheric concentration of radon progeny at the time of sampling
The method consists of initially collecting a sample of airborne radon progeny by using a portable air pump to draw air through a low-porosity filter. The radon progeny that are present in the air attach to the inlet face of the filter used. These progeny subsequently decay, emitting alpha particles and other forms of radiation in the process. During this decay, the emissions of alpha particles are detected and counted, using an instrument (an alpha counter) designed and manufactured for that purpose.
The counting results obtained are then used along with other pertinent data and observations to estimate the concentration, in units called working levels (WLs). The concentration of radon progeny is calculated from the alpha disintegrations per WL over the interval between the end of sampling and the middle of alpha counting. It considers the volume of air sampled, the alpha activity of collected and resultant radon progeny, the efficiency and background of the alpha counter, and the absorption characteristics of the filter used during sampling.
Air sampling locations should be selected to accurately reflect the conditions to be assessed. Non‑representative or adverse sampling conditions, such as areas of turbulent air flow (e.g., duct exhausts, junctures or intersections of ventilation passageways, door or window openings) should be avoided. When collecting radon progeny samples for the purpose of estimating or confirming radiation doses to workers, the actual atmospheres breathed by the respective workers should be sampled where possible. Such samples may be collected, for example, at the individuals’ workstations over a representative period. Alternatively, if concentrations of airborne radon progeny are similar over a large area, it may suffice to collect representative samples while moving through the area, or at appropriate points within the area. The latter approach may be particularly appropriate within uranium processing plants and in travel ways and/or similar areas of mines.
Samples that are intended to aid in the planning, development and evaluation of engineering works and production processes should be representative of the conditions that they are intended to assess. Accordingly, these samples should be collected at appropriate locations and times. For example, to determine the impact of modifications to mine or building ventilation systems, or to guide the installation of such systems, it may be necessary to collect several air samples at multiple locations before, after and during the changes.
G.4 Ascertaining Doses from Radon Gas
The effective dose resulting from the inhalation of Rn-222 gas alone may be ascertained by multiplying the Rn-222 intake by the effective dose coefficient. It may also be ascertained by multiplying the Rn-222 concentration by the occupancy time and the effective dose rate per unit concentration factor. This factor is the effective dose rate due to a chronic exposure to a concentration of 1 Bq/m3 of Rn-222 gas, once the radon has reached equilibrium in organs and tissues. The recommended values for these parameters, as well as the ALI, are presented in table G.1 [42].
| Parameter | Value | Units |
|---|---|---|
| Effective dose coefficient | 4.4 × 10-10 | Sv/Bq |
| Effective dose rate per unit concentration factor | 1.8 × 10-7 | mSv/(Bq·h·m-3) |
| ALI | 45.5 | MBq |
Glossary
For definitions of terms used in this document, see REGDOC‑3.6, Glossary of CNSC Terminology, which includes terms and definitions used in the Nuclear Safety and Control Act and the regulations made under it, and in CNSC regulatory documents and other publications. REGDOC‑3.6 is provided for reference and information.
References
- Canadian Nuclear Safety Commission (CNSC), REGDOC-2.7.1, Radiation Protection, Ottawa, 2021.
- CNSC, REGDOC-2.7.2, Dosimetry, Volume II: Technical and Management System Requirements for Dosimetry Services , Ottawa, 2020.
- CNSC, REGDOC‑2.9.1, Environmental Principles, Assessments and Protection Measures, Ottawa, 2017.
- International Commission on Radiological Protection (ICRP), Publication 103, The 2007 Recommendations of the International Commission on Radiological Protection , Annals of the ICRP, Vol. 37, Nos. 2‒4, Oxford, 2007.
- International Commission on Radiation Units and Measurements (ICRU), Report 51, Quantities and Units in Radiation Protection Dosimetry, Bethesda, Maryland, 1993.
- American National Standards Institute/Health Physics Society, ANSI/HPS N13.41-2011 (R2018), Criteria for Performing Multiple Dosimetry, 2018.
- International Atomic Energy Agency (IAEA), TECDOC-1731, Implications for Occupational Radiation Protection of the New Dose Limit for the Lens of the Eye , Vienna, 2013.
- CNSC, Radionuclide Information Booklet , Ottawa, 2018.
- IAEA, TECDOC-1162, Generic Procedures for Assessment and Response During a Radiological Emergency , Vienna, 2000.
- Kocher, D. C., and K. F. Eckerman, “Electron Dose-Rate Conversion Factors for External Exposure of the Skin from Uniformly Deposited Activity on the Body Surface,” Health Physics, Vol. 53, No. 2, pp. 135–141, 1987.
- ICRP, Publication 119, Compendium of Dose Coefficients Based on ICRP Publication 60 , Vol. 41, Supplement 1, Oxford, 2012.
- ICRU, Report 69, Direct Determination of the Body Content of Radionuclides, Bethesda, Maryland, 2016.
- ICRP, Publication 130, Occupational Intakes of Radionuclides: Part I, Vol. 44, No. 2, 2015.
- IAEA, Safety Series No. 114, Direct Methods for Measuring Radionuclides in the Human Body , Vienna, 1996.
- ICRP, Publication 66, Human Respiratory Tract Model for Radiological Protection, Vol. 24, Nos. 1–3, 1994.
- Strom, D. J., and P. S. Stansbury, “Minimum Detectable Activity When Background Is Counted Longer Than the Sample,” Health Physics, Vol. 63, No. 3, pp. 360–361, 1992.
- United States Environmental Protection Agency, Multi-Agency Radiological Laboratory Analytical Protocols Manual (MARLAP) , EPA 402-B-04-001A, July 2004
- International Organization for Standardization, ISO 20553:2006 (R2015), Radiation Protection – Monitoring of Workers Occupationally Exposed to a Risk of Internal Contamination with Radioactive Material , 2006.
- Hickey, E. E., et al, NUREG‑1400, Air Sampling in the Workplace, 1993.
- Castellani, C. M., et al., EURADOS Report 2013-01, IDEAS Guidelines (Version 2) for the Estimation of Committed Doses from Incorporation Monitoring Data, 2013.
- IAEA, Safety Reports Series No. 37, Methods for Assessing Occupational Radiation Doses Due to Intakes of Radionuclides , Vienna, 2004.
- ICRP, Publication 95, Doses to Infants from Ingestion of Radionuclides in Mothers’ Milk, Vol. 34, Nos. 3–4, 2004.
- ICRP, Publication 100, Errata to: Doses to Infants from Ingestion of Radionuclides in Mothers’ Milk (ICRP Publication 95, Ann. ICRP 34(3/4)) , 2007.
- National Council on Radiation Protection and Measurements (NCRP), Report No. 156, Development of a Biokinetic Model for Radionuclide-Contaminated Wounds and Procedures for Their Assessment, Dosimetry and Treatment , 2006.
- ICRP, Publication 78, Individual Monitoring for Internal Exposure of Workers: Replacement of ICRP Publication 54, Vol. 27, Nos. 3–4, 1997.
- International Organization for Standardization, ISO 27048: 2011 (R2016), Radiation Protection – Dose Assessment for the Monitoring of Workers for Internal Radiation Exposure, 2011.
- Toohey, R. E., et al., “Dose Coefficients for Intakes of Radionuclides via Contaminated Wounds,” Health Physics, Vol. 100, No. 5, 2011.
- Health Physics Society, ANSI/HPS N13.39–2001, Design of Internal Dosimetry Programs, McLean, Virginia, 2011.
- ICRP, Publication 67, Age-Dependent Doses to Members of the Public from Intake of Radionuclides: Part 2 – Ingestion Dose Coefficients , Vol. 23, Nos. 3–4, 1993.
- ICRP, Publication 69, Age-Dependent Doses to Members of the Public from Intake of Radionuclides: Part 3 – Ingestion Dose Coefficients , Vol. 25, No. 1, 1995.
- Health and Welfare Canada, Bioassay Guideline 2 - Guidelines for Tritium Bioassay, Report of the Working Group on Bioassay and In Vivo Monitoring Criteria , Environmental Health Directorate, 83‑EHD-87, 1983.
- Kramer, G. H., and S. Yiu, “The Canadian National Calibration Reference Centre for In-Vivo Monitoring: Thyroid Monitoring. Part VI: Choosing a Detector for Either I-125 and/or I‑131,” Canadian Journal of Medical Radiation Technology, Vol. 27, No. 2, 1996.
- Burns, L. C., et al., The Thyroid Intercomparison Program, Human Monitoring Laboratory Technical Report, HMLTD-88–3, Health Canada, 1996, Ottawa.
- Kramer, G. H., and D. P. Meyerhof, “The Canadian National Calibration Reference Centre for In‑Vivo Monitoring: Thyroid Monitoring Part III: A Basic Calibration Procedure for Thyroid Monitoring,” Canadian Journal of Medical Radiation Technology, Volume 25, No. 2, 1994.
- ICRP, Publication 107, Nuclear Decay Data for Dosimetric Calculations, Vol. 38, No. 3, 2008.
- National Institute of Standards and Technology, Physical Measurement Laboratory, Atomic Weights and Isotopic Compositions, available at http://www.nist.gov/pml/data/comp.
- SENES Consultants, Evaluation of Default Annual Limit on Intake (ALI) for Yellowcake and Uranium Ore, CNSC-RSP-0297, 2013.
- International Organization for Standardization, ISO 16638-1, Radiological Protection – Monitoring and Internal Dosimetry for Specific Materials – Part 1: Inhalation of Uranium Compounds , 2015.
- CNSC, RSP-0165, Uranium Intake – Dose Estimation Methods, 2003.
- ICRP, Publication 65, Protection Against Radon-222 at Home and at Work, Vol. 23, No. 2, 1993.
- ICRP, Publication 60, 1990 Recommendations of the International Commission on Radiological Protection, Vol. 21, No. 1–3, 1991.
- ICRP, Publication 137, Occupational Intakes of Radionuclides: Part 3, Vol. 46, Nos. 3–4, 2017.
Additional Information
The following documents provide additional information that may be relevant and useful for understanding the guidance provided in this regulatory document:
- Advisory Committee on Radiological Protection, ACRP‑17, Report on External Occupational Dosimetry in Canada, 1995.
- American National Standards Institute, ANSI/HPS N13.30-2011 (R2017), Performance Criteria for Radiobioassay, 2017.
- American National Standards Institute/Health Physics Society, ANSI/HPS N.13.41, Criteria for Performing Multiple Dosimetry, Washington, 1997.
- Becker, D. V., et al., Society of Nuclear Medicine Procedure Guideline for Thyroid Uptake Measurement, Society of Nuclear Medicine, Version 2.0, Reston, Virginia, 1999.
- Birchall, A., et al., “IMBA Professional Plus: A Flexible Approach to Internal Dosimetry,” Radiation Protection Dosimetry, Vol. 125, Nos. 1–4, pp. 194–197, 2007.
- Christensen, P., H. W. Julius, and T.O. Marshall, “Implication of New CEC Recommendations for Individual Monitoring for External Radiation Doses to the Skin and the Extremities,” Radiation Protection Dosimetry, Vol. 39, pp. 91–94, Oxford, 1991.
- Faulkner, K., and R. M. Harrison, “Estimation of Effective Dose Equivalent to Staff in Diagnostic Radiology,” Physics in Medicine and Biology, No. 33, Institute of Physics, Philadelphia, 1988.
- International Atomic Energy Agency (IAEA), TECDOC-869, Assessment and Treatment of External and Internal Radionuclide Contamination, Vienna, 1996.
- Kramer, G. H., and S. Yiu, “Examination of the Effect of Counting Geometry on I–125 Monitoring Using MCNP,” Health Physics, Vol. 72, No. 3, 1997.
- National Council on Radiation Protection and Measurements, NCRP Report No. 122: Use of Personal Monitors to Estimate Effective Dose Equivalent and Effective Dose to Workers for External Exposure to Low-LET Radiation , Bethesda, MD, 1995
- Reece, W.D., et al., NUREG/CR-4297, Extremity Monitoring: Considerations for Use, Dosimeter Placement, and Evaluation, United States Nuclear Regulatory Commission, Washington, 1985.
- Rosenstein, M., and E. W. Webster, “Effective Dose to Personnel Wearing Protective Aprons During Fluoroscopy and Interventional Radiology,” Health Physics, Vol. 67, pp. 88–89. Philadelphia, 1994.
CNSC Regulatory Document Series
Facilities and activities within the nuclear sector in Canada are regulated by the CNSC. In addition to the Nuclear Safety and Control Act and associated regulations, these facilities and activities may also be required to comply with other regulatory instruments such as regulatory documents or standards.
CNSC regulatory documents are classified under the following categories and series:
1.0 Regulated facilities and activities
Series
- 1.1 Reactor facilities
- 1.2 Class IB facilities
- 1.3 Uranium mines and mills
- 1.4 Class II facilities
- 1.5 Certification of prescribed equipment
- 1.6 Nuclear substances and radiation devices
2.0 Safety and control areas
Series
- 2.1 Management system
- 2.2 Human performance management
- 2.3 Operating performance
- 2.4 Safety analysis
- 2.5 Physical design
- 2.6 Fitness for service
- 2.7 Radiation protection
- 2.8 Conventional health and safety
- 2.9 Environmental protection
- 2.10 Emergency management and fire protection
- 2.11 Waste management
- 2.12 Security
- 2.13 Safeguards and non‑proliferation
- 2.14 Packaging and transport
3.0 Other regulatory areas
Series
- 3.1 Reporting requirements
- 3.2 Public and Indigenous engagement
- 3.3 Financial guarantees
- 3.4 Commission proceedings
- 3.5 CNSC processes and practices
- 3.6 Glossary of CNSC terminology
Note: The regulatory document series may be adjusted periodically by the CNSC. Each regulatory document series listed above may contain multiple regulatory documents. Visit the CNSC’s website for the latest list of regulatory documents.
Footnotes
- Footnote 1
-
The NDR is a registry of occupational doses to Canadian workers. The NDR also includes doses received by foreign workers; however, these doses are not used for analyses of the NDR data. They are included so that dosimetry services can comply with section 19 of the RPR.
- Footnote 2
-
Pulsed radiation fields are characterized by dose rates periodically varying in intensity with time.
- Footnote 3
-
For persons who are less than 18 years of age, the committed equivalent dose is the equivalent dose received by an organ or tissue from a radionuclide from the time of intake to age 70 years.
- Footnote 4
-
For persons who are less than 18 years of age, the CED is the effective dose received from the time of intake to age 70 years.
- Footnote 5
-
The ICRP classifies inhaled particulates into 3 types, depending on their rate of absorption into blood from the lungs. Type F particulates are fast-clearing, being retained in the respiratory tract with a biological half-life of less than 1 hour. Materials classified as Type M follow a moderate clearance rate from the respiratory tract (typically 90% of the inhaled particulates have a biological half-life of about 100 days), while Type S materials are slow‑clearing and may be retained in the respiratory tract for periods exceeding 1 year (typically 99.9% of the inhaled Type S particulates have a biological half-life of about 7,000 days). The chemical characteristics of a compound determine its absorption type.
- Footnote 6
-
Current ICRP biokinetic models can be found in ICRP Publication 67 [29] and 69 [12], for example, or more recent models when published.
- Footnote 7
-
Absorption of radionuclides from the respiratory tract to blood is described using fr, which is the fraction of the activity deposited in the respiratory tract that dissolves rapidly, at a rate sr (d-1). The remainder of the activity deposited in the respiratory tract dissolves more slowly, at a rate ss (d-1), as per ICRP Publication 66, Human Respiratory Tract Model for Radiological Protection [15].
- Footnote 8
-
The ratio for Po-210 may be used for conservatively estimating the dose from radon progeny.
- Footnote 9
-
Assuming elemental iodine vapour.
Page details
- Date modified: